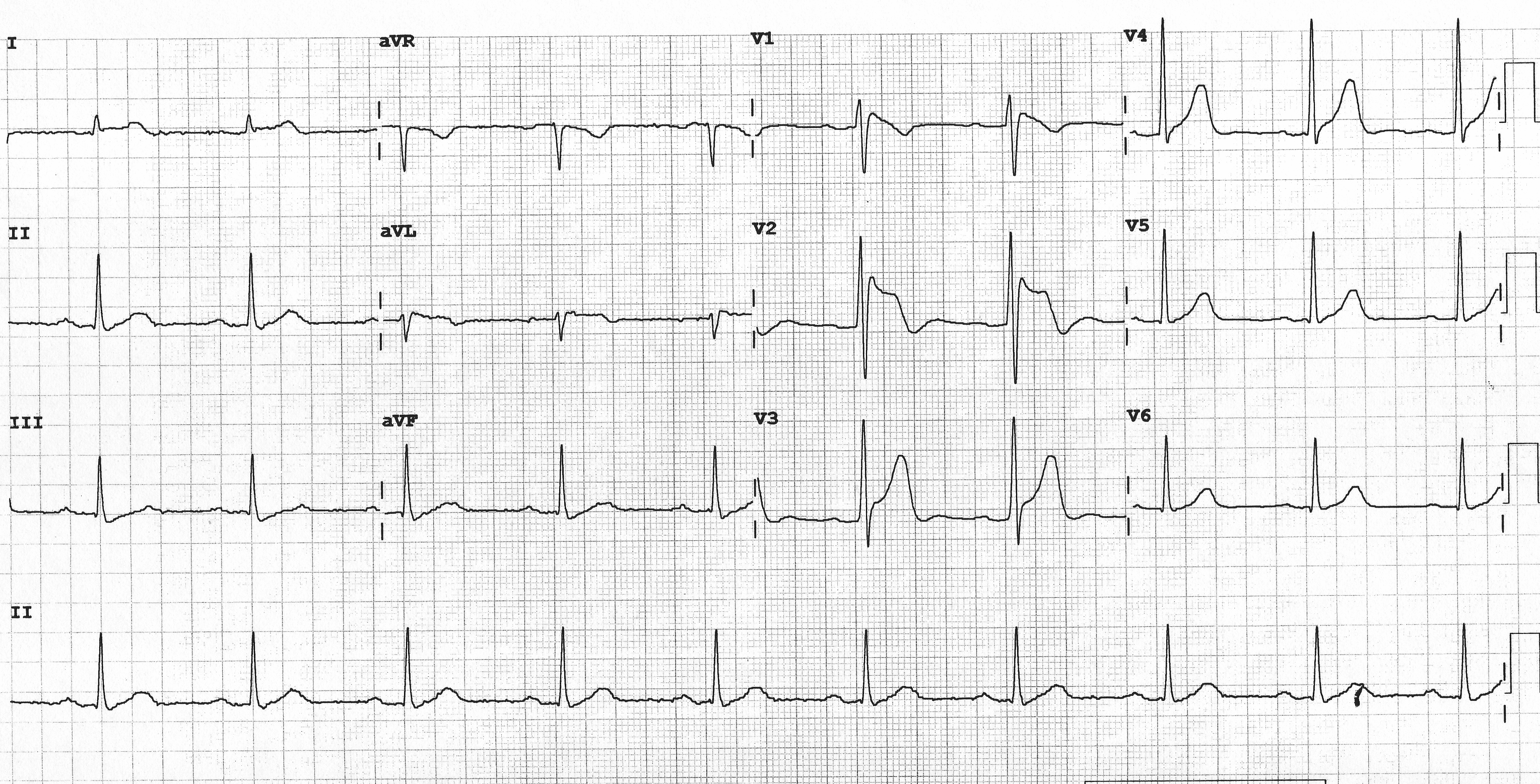
A 44 y/o male presents to the Emergency room with a 2-day history of flank pain and fever
with minor pleuritic chest pain prompting the emergency room physician to request the ECG shown.
He is febrile (38.8°C) and has leukocytosis and likely pyelonephritis. He has no personal
or family history of sudden death or related concerning events.
Which of the following actions is preferred?
- Administer antipyretics.
- Start Isoproterenol infusion.
- Start oral quinidine.
- Admit for EP study.
- Admit for ICD implantation.
Show Answer
Answer: A
ECG shows typeI Brugada pattern. Fever is a known trigger for both clinical events
and worsening ECG findings in Brugada Syndrome patients, and represents a medical emergency
that should be treated with urgent antipyretics.
Active/recurrent ventricular arrhythmia in Brugada Syndrome is best treated with
quinidine or catheter ablation, but this patient is asymptomatic
and without arrhythmias.
EP testing is a 2B recommendation and generally discouraged.
ICDs are generally not indicated in asymptomatic Brugada Syndrome patients.
| Recommendations for Brugada Syndrome |
Class |
|
Asymptomatic, type I ECG: Observation w/o specific Tx.
|
I |
|
Spontaneous type I ECG + SCA/VA/Syncope: ICD.
|
I |
|
Recurrent ICD shocks for polymorphic VT: Quinidine or Ablation.
|
I |
|
Symptomatic spontaneous type I ECG + not ICD candidate or refuse: Quinidine or Ablation.
|
I |
|
Suspected Brugada but w/o spontaneous type I: pharmacological challenge.
|
IIa |
|
EP study in asymptomatic spontaneous type I.
In asymptomatic patient, the prognostic value of Ep study is low.
In symptomatic patient, positive EP study does not add anything to the
evaluation of the patient as an ICD is warranted.
|
IIb |
|
Genetic testing in relatives.
Yield of genetic testing in phenotype positive = 20-30%.
Negative testing does not exclude Brugada syndrome.
|
IIb |
![]()