Answer: A
Fluoxetine is CYP2C9 inhibitor.
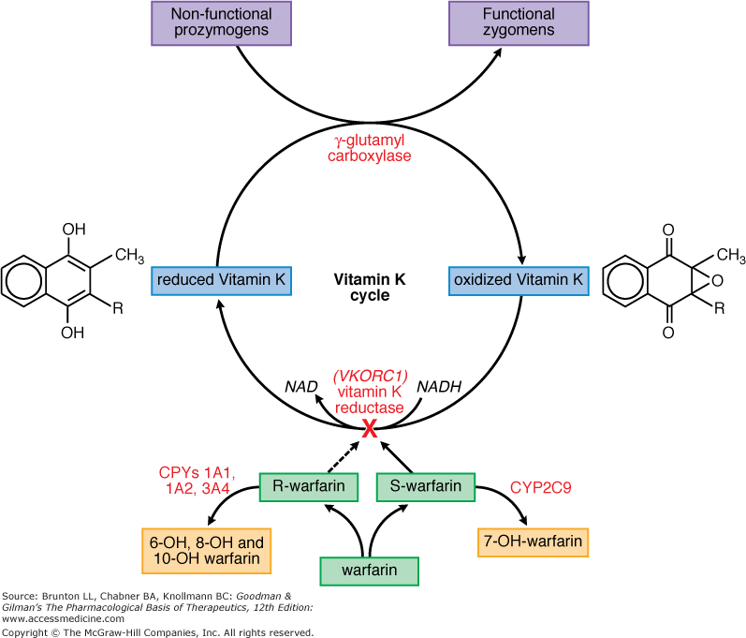
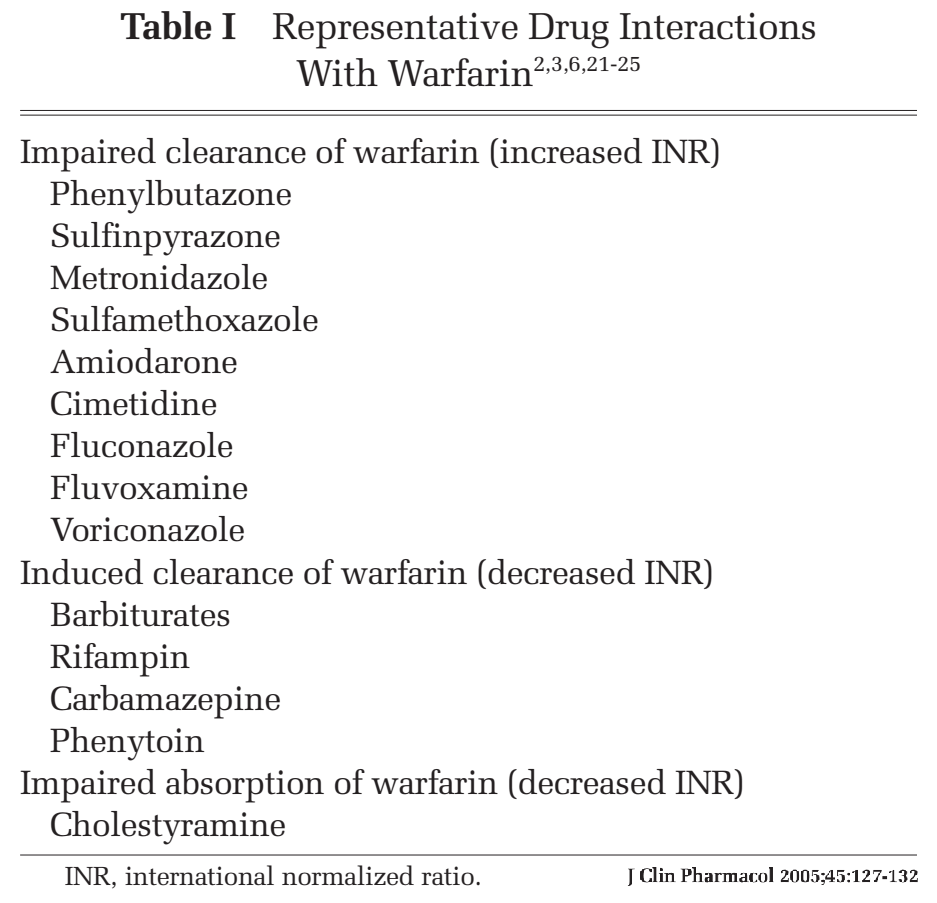 Warfarin is mainly metabolized by CYP2C9. Drugs such as SSRI and amiodarone inhibit CYP2C9, while
rifampin and dilantin are inducers.
Warfarin is mainly metabolized by CYP2C9. Drugs such as SSRI and amiodarone inhibit CYP2C9, while
rifampin and dilantin are inducers.
Variance in warfarin dosing is associated with polymorphisms of CYP2C9 and VKORC1.
Asians are required lower warfarin dosing mainly due to VKORC1 'A' allele.
Variance in warfarin dosing is associated with polymorphisms of CYP2C9 and VKORC1.
Asians are required lower warfarin dosing mainly due to VKORC1 'A' allele.
RELATED:
NOACs and PGP
- PGP = P-Glycoprotein = gate-keeper in enterocytes, hepatocytes, and renal cells.
- All NOACs are PGP substrates; dabigatran being strongest.
- Strong PGP inhibotors: dronedarone > amiodarone.
- Strong PGP inhibotors: CCB: nicardipine > verapamil > diltiazem >nifedipine.
- Other strong PGP inhibitors: Azole group, protease inhibitors, cyclosporin.
- PGP inducers: rifampin.
NOACs and CYP3A4
- Except dabigatran, all NOACs are metabolized through CYP3A4.
- Strong CYP3A4 inhibotors: Azole group, protease inhibitors.
- Moderate CYP3A4 inhibotors: fluconazole, erythromycin/clarithromycin.
- strong PGP and CYP3A4 inhibitors: dronedarone, Azole group (except fluconazole), protease inhibitors.