 1st degree AV block. In a severe case (PR>330ms), symptoms similar to pacemaker syndrome
may occur.
1st degree AV block. In a severe case (PR>330ms), symptoms similar to pacemaker syndrome
may occur.
 Mobitz I or Wenckebach. Pacemaker is indicated if symptomatic.
Mobitz I or Wenckebach. Pacemaker is indicated if symptomatic.
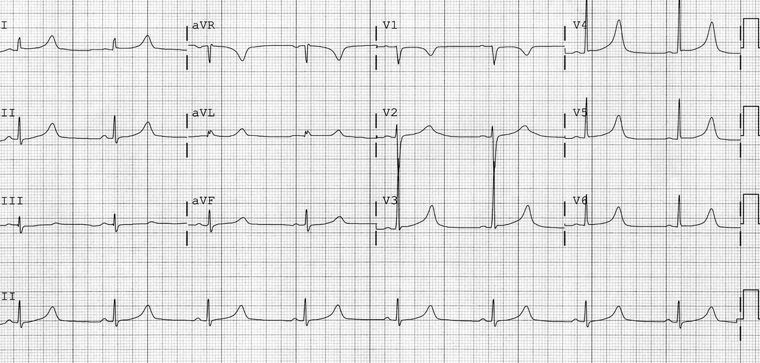
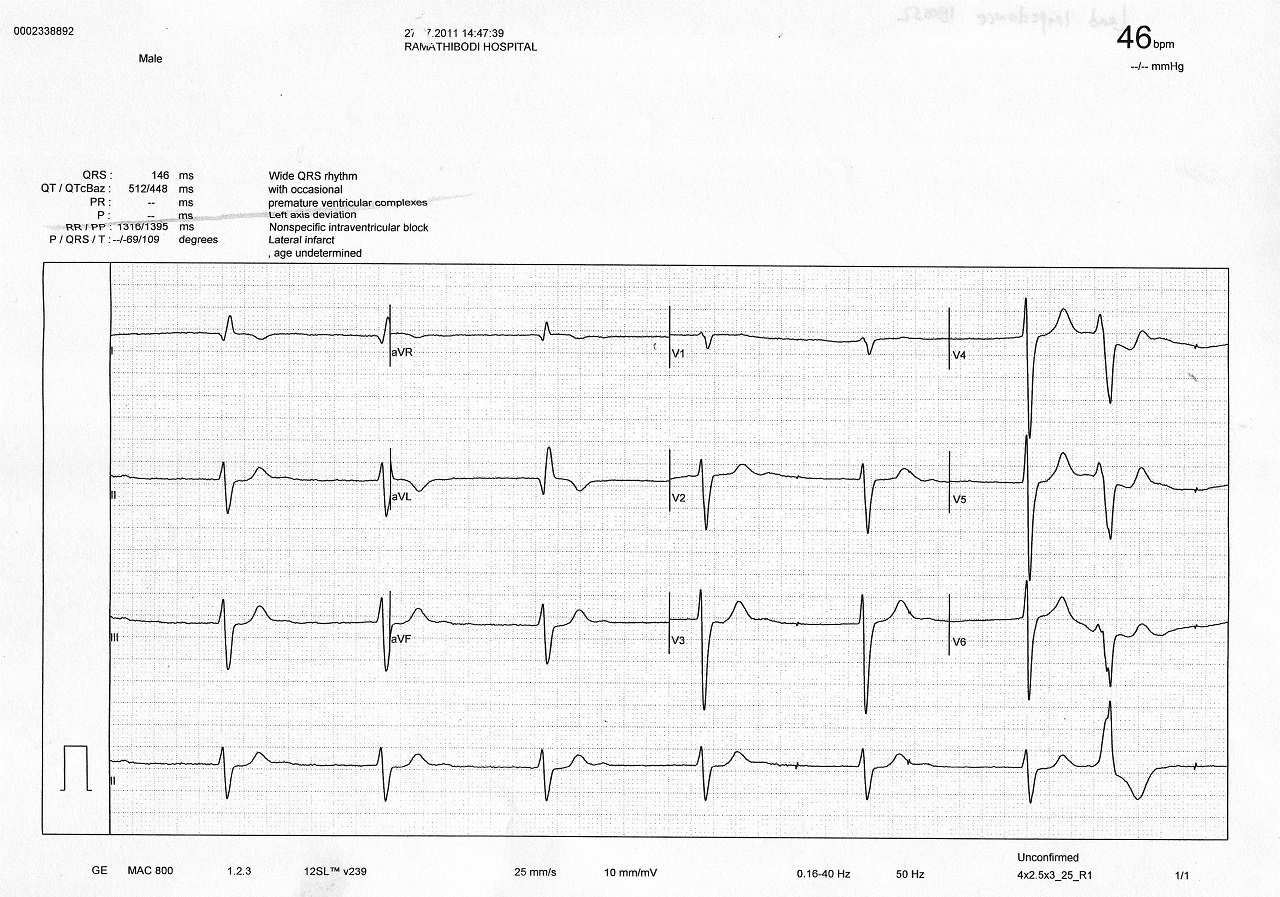
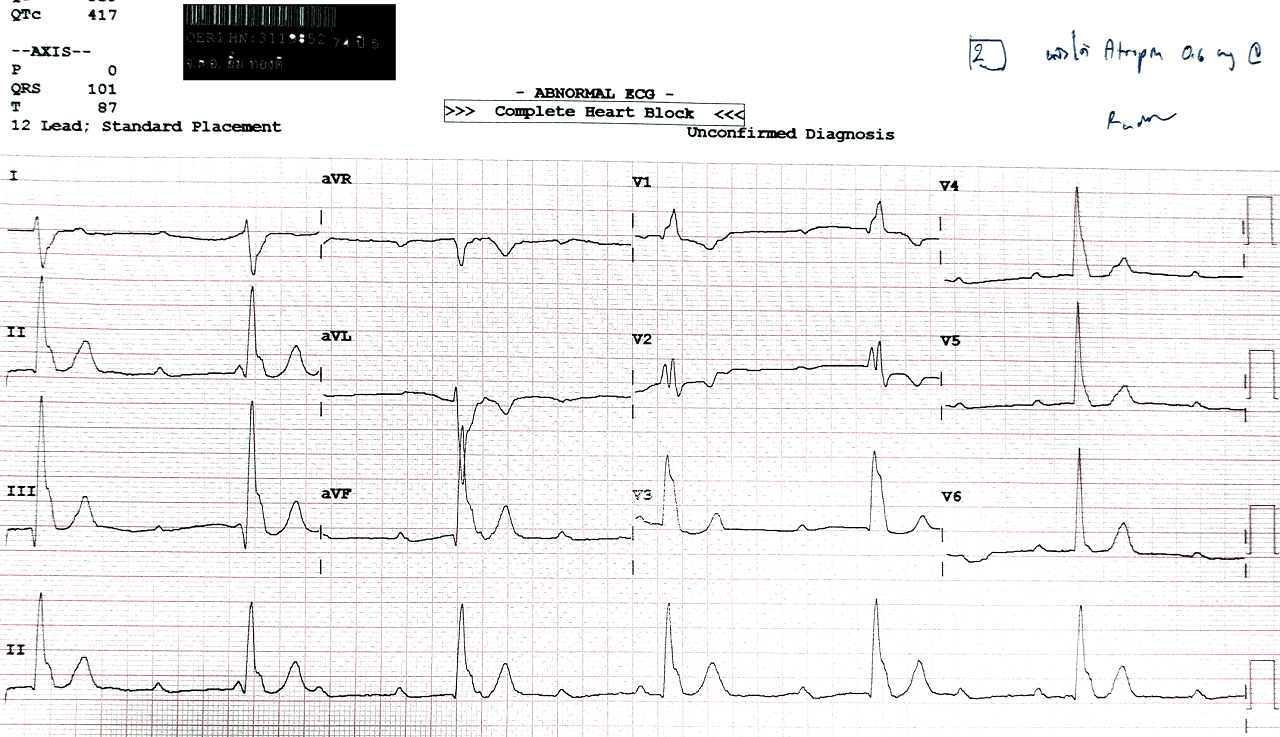 Complete heart block. Escape rate is slow with RBBB and LPFB morphology.
Complete heart block. Escape rate is slow with RBBB and LPFB morphology.
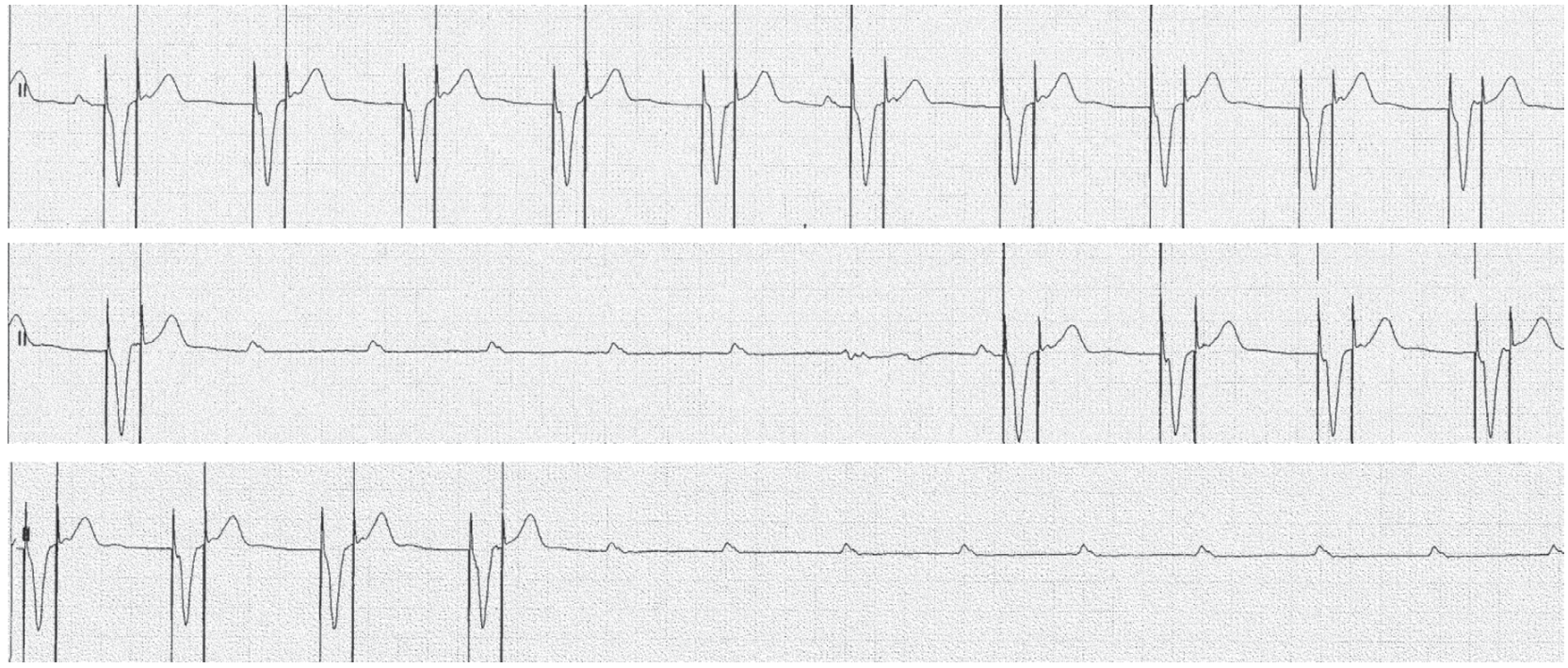
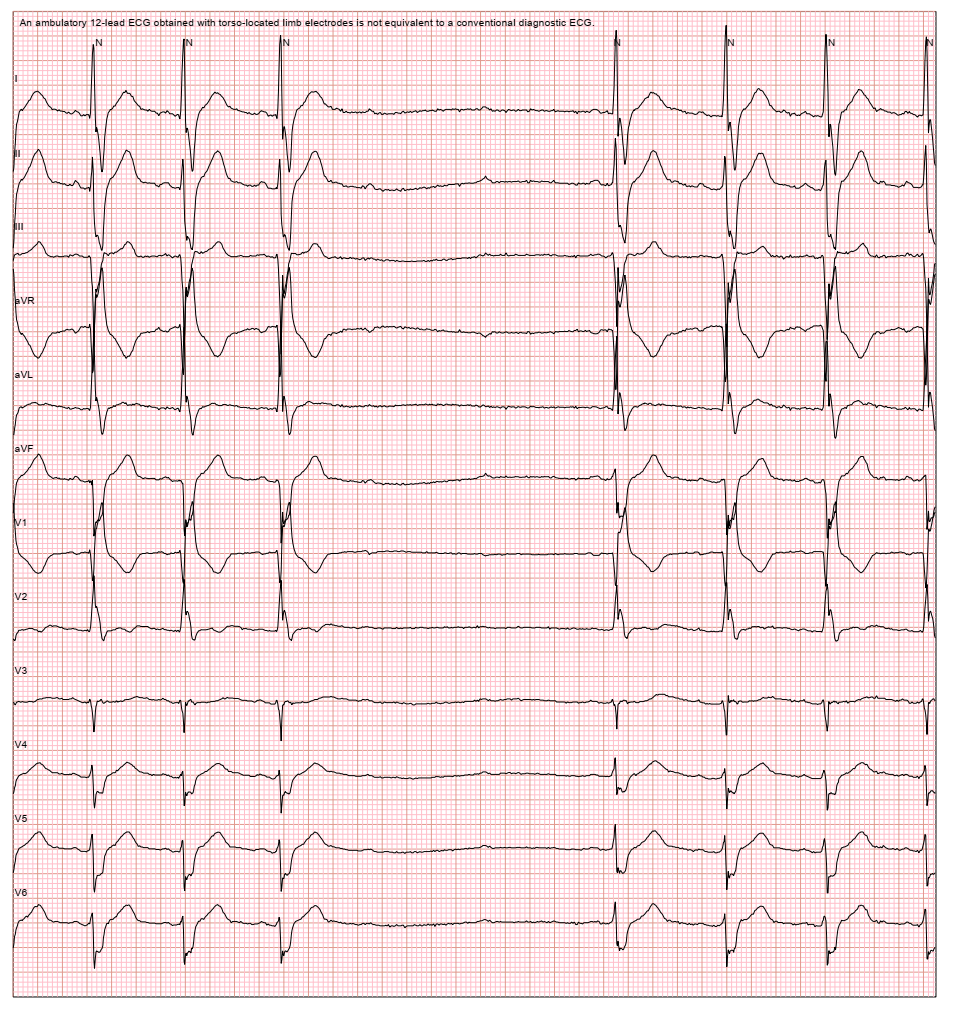 Intermittent complete heart block. 2Ps without any QRS. Underlying
rhythm is sinus rhythm with RBBB and LAFB.
Intermittent complete heart block. 2Ps without any QRS. Underlying
rhythm is sinus rhythm with RBBB and LAFB.
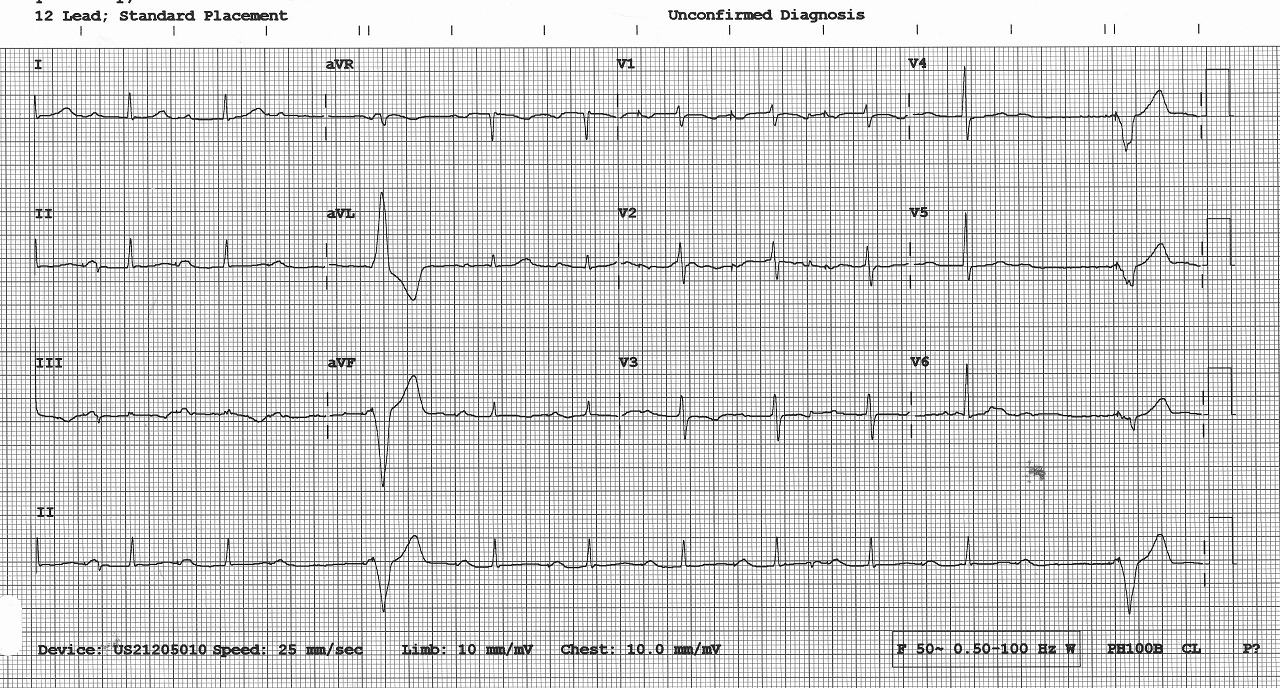
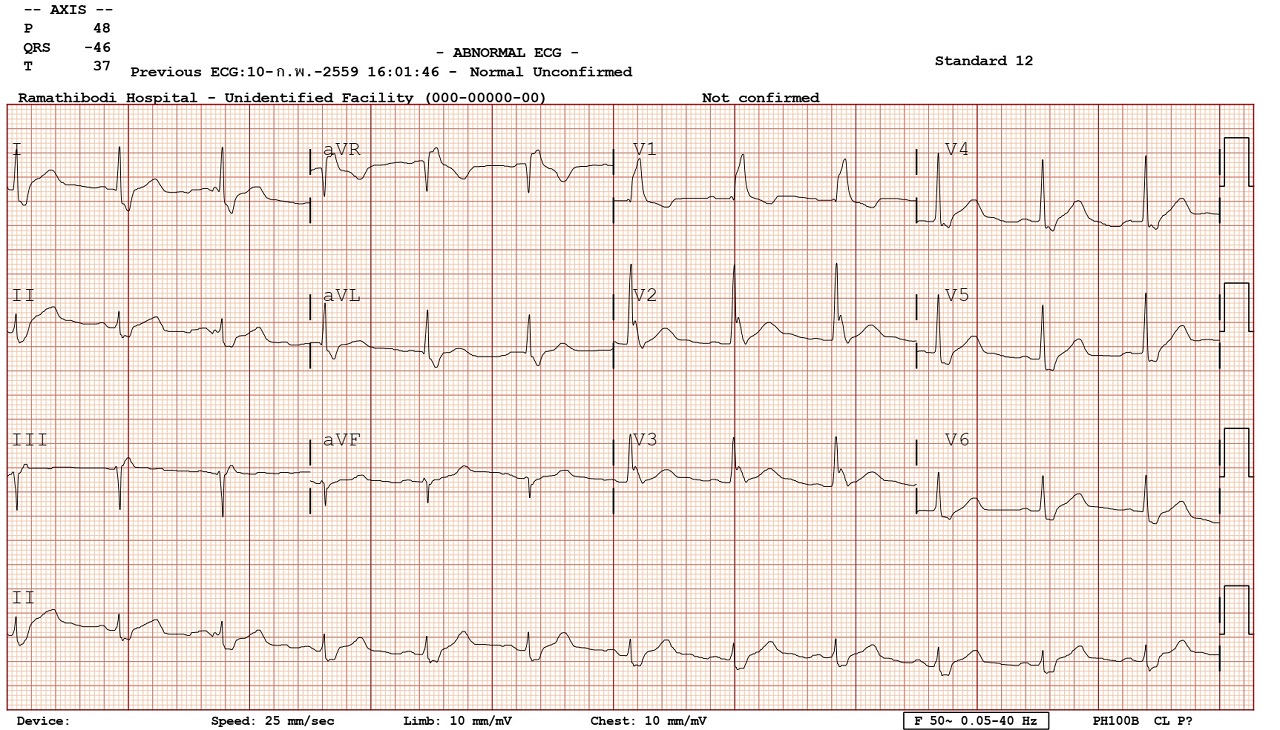 Bifascicular block with 1st degree AV block. Consider pacemaker if
HV ≥70ms, evidence of infranodal block, or alternating BBB.
Bifascicular block with 1st degree AV block. Consider pacemaker if
HV ≥70ms, evidence of infranodal block, or alternating BBB.
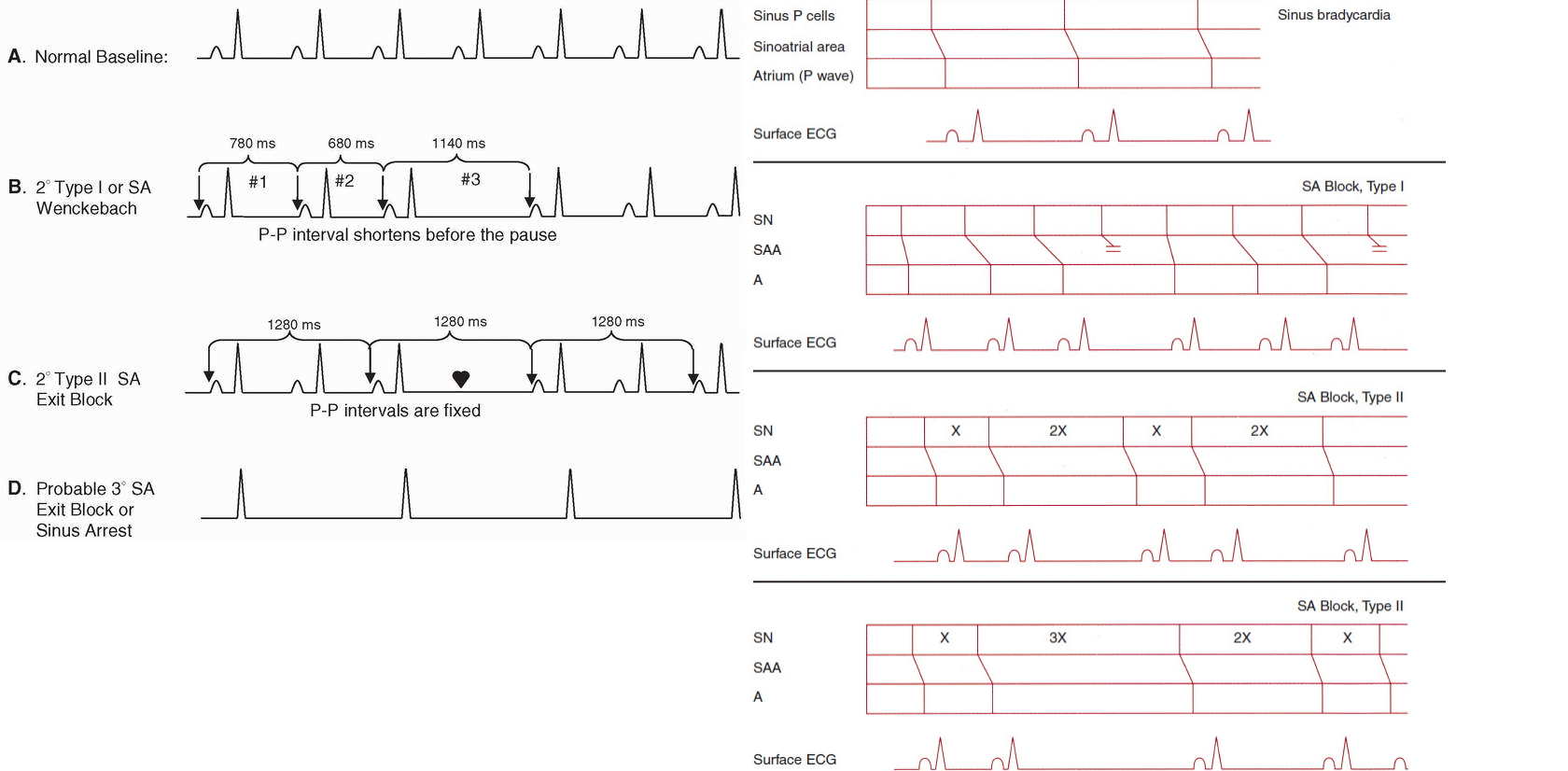
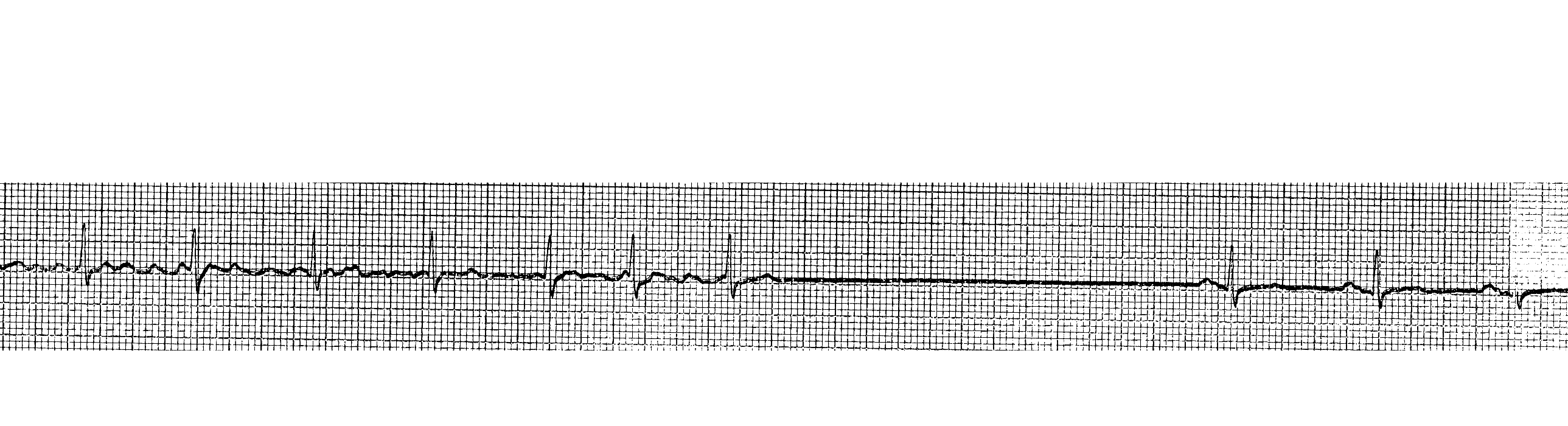
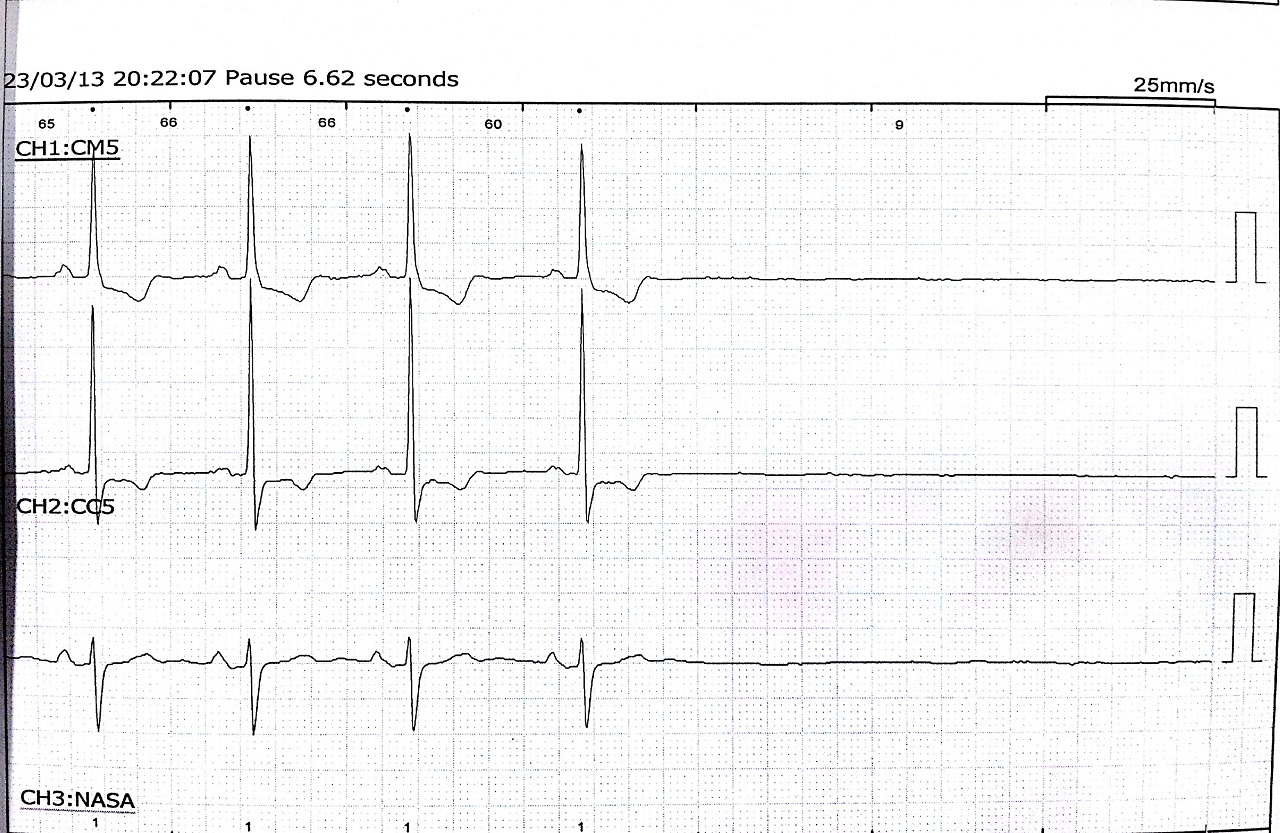 Sinus pause
Sinus pause
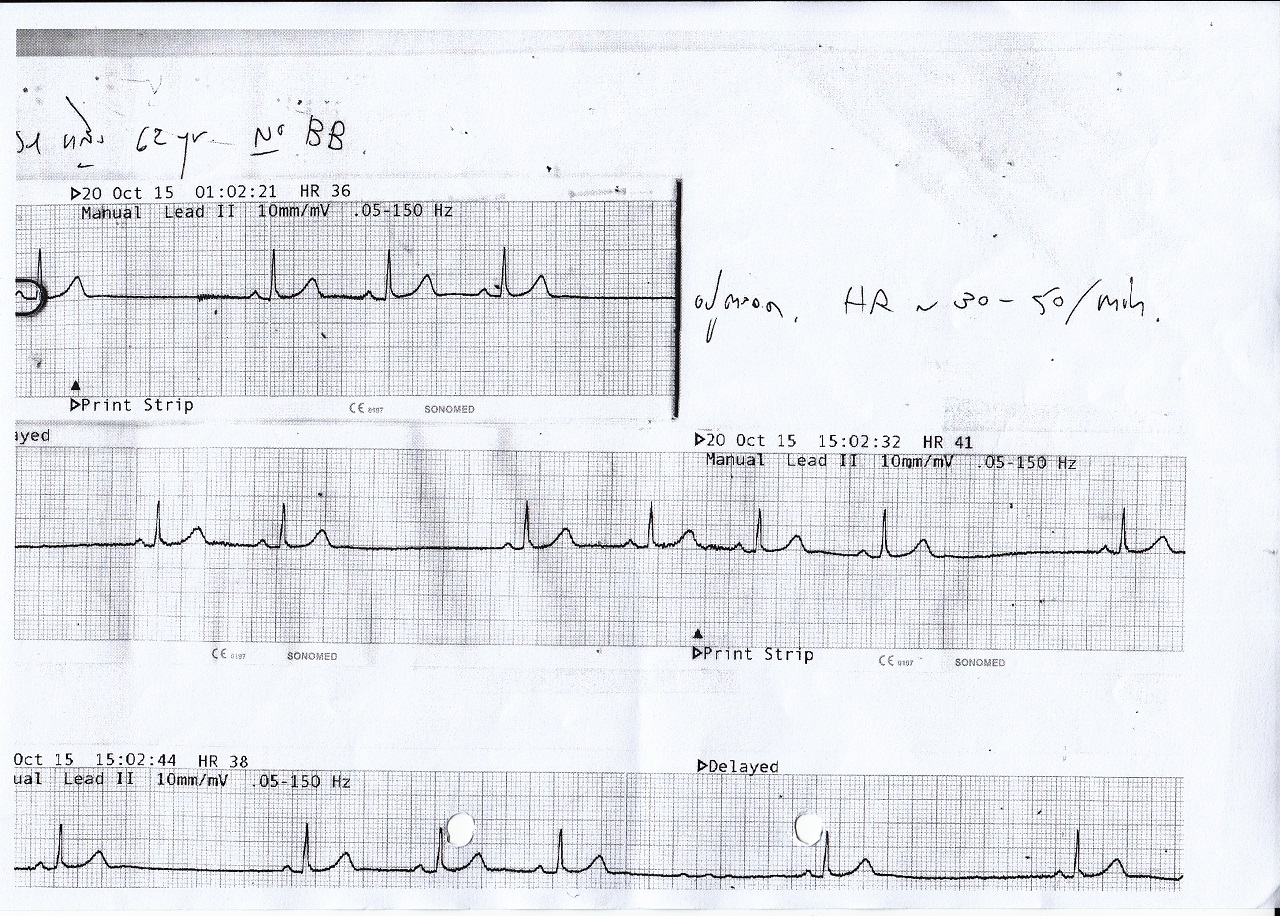
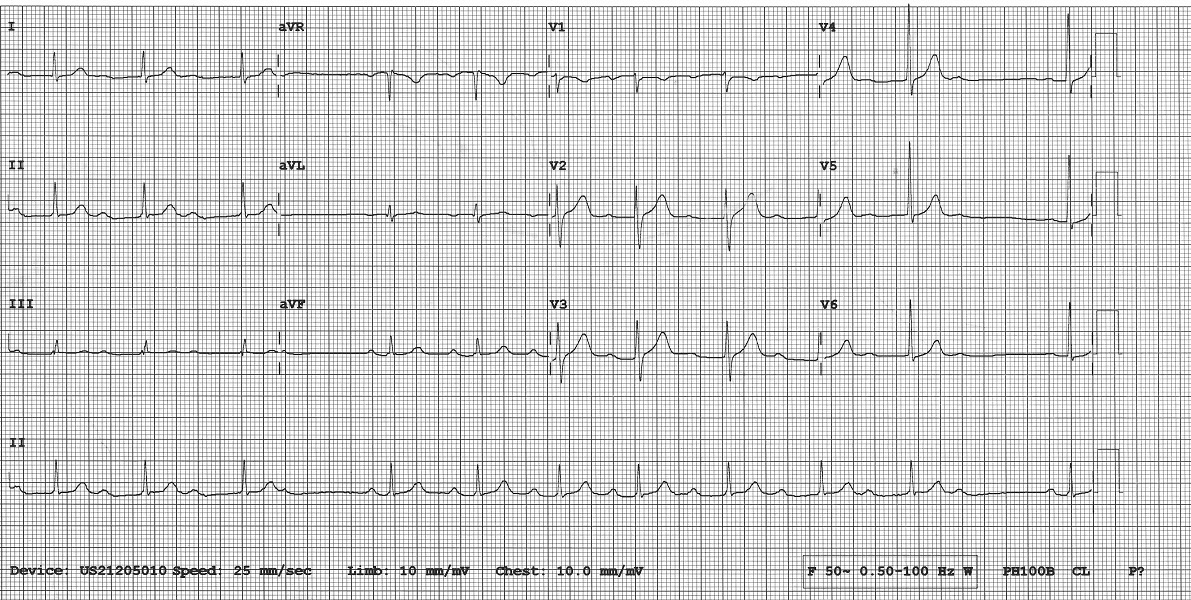
 AF with conversion pause
AF with conversion pause
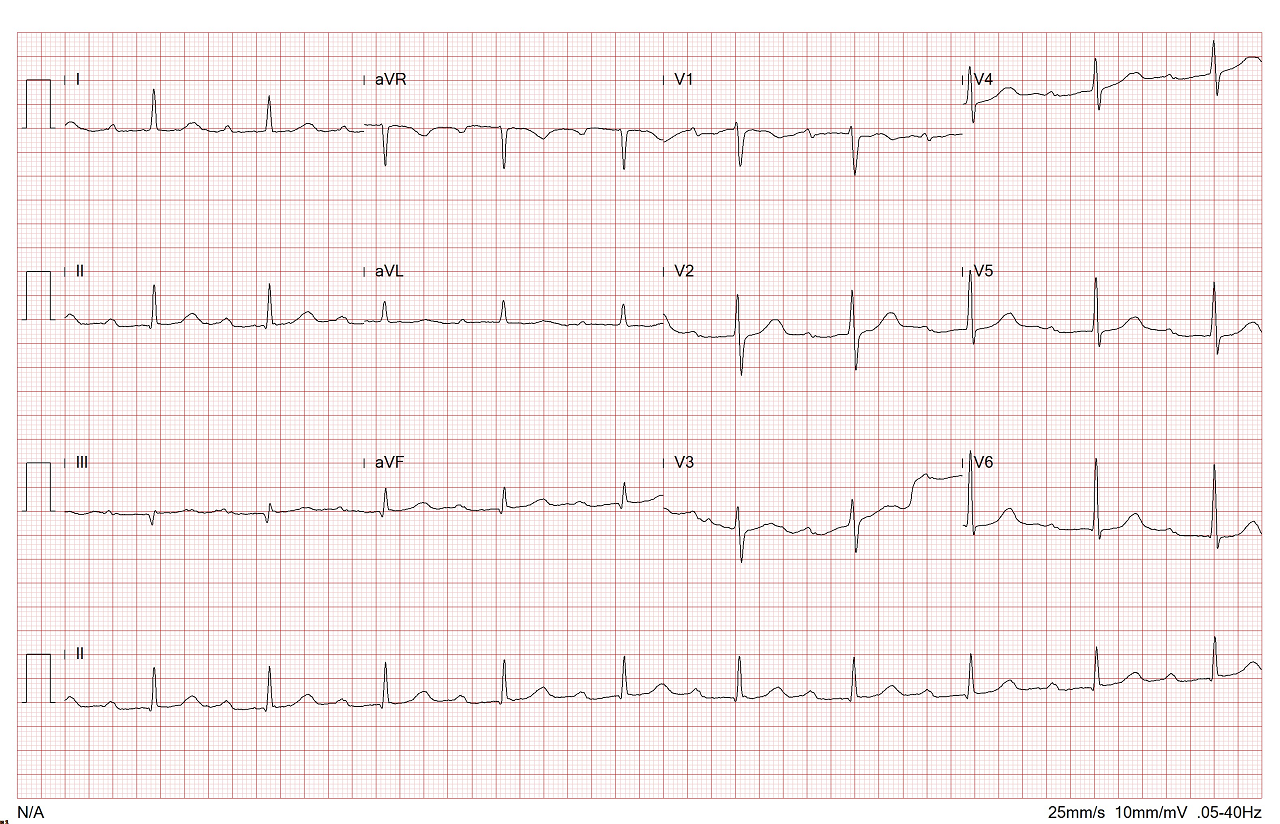
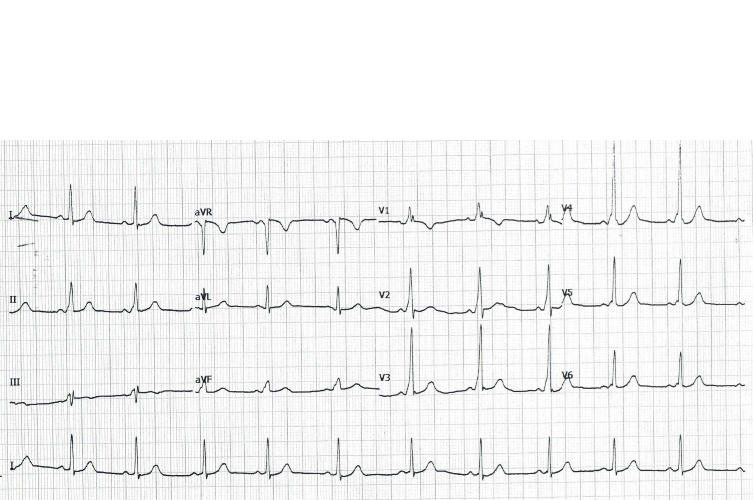
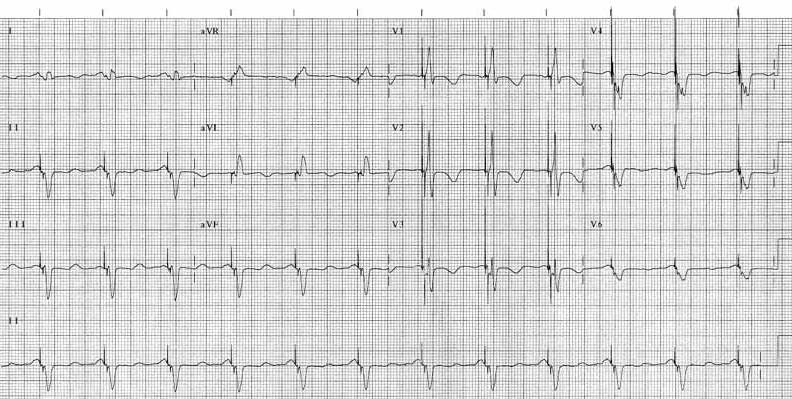
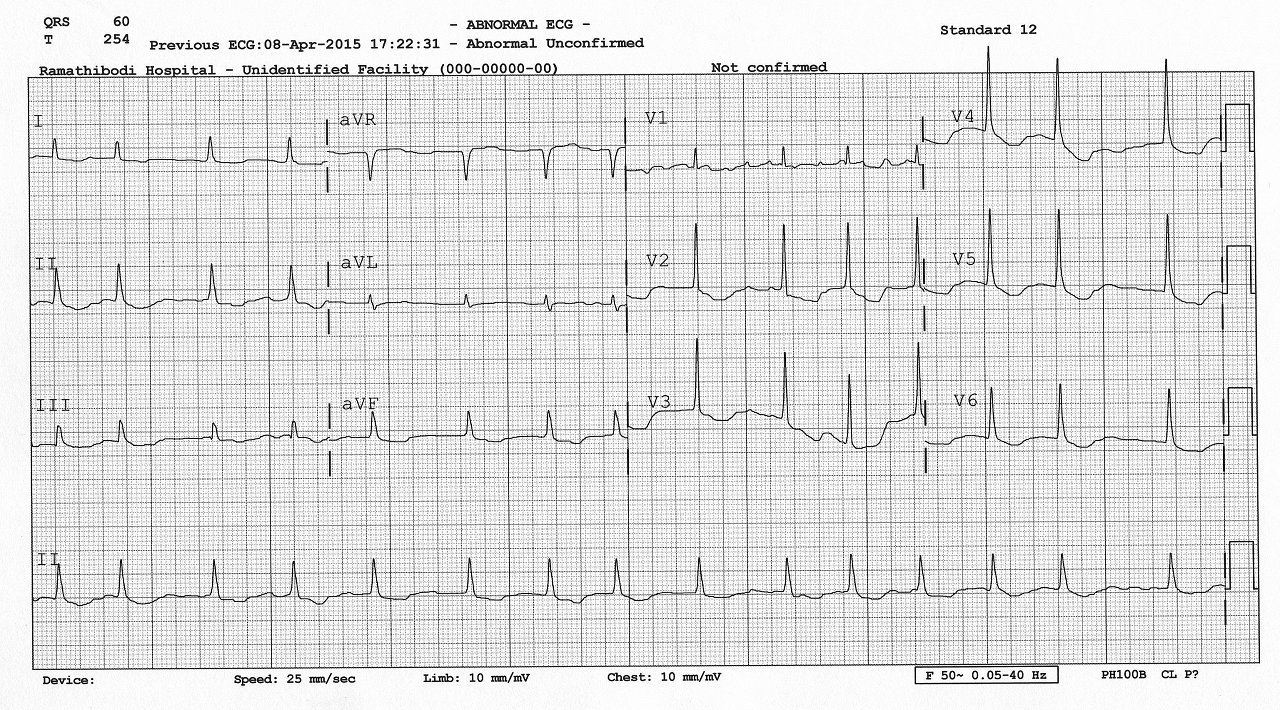 Atrial Fibrillation: irregularly irregular rhythm. Noted with fibrillatory waves in V1.
Atrial Fibrillation: irregularly irregular rhythm. Noted with fibrillatory waves in V1.
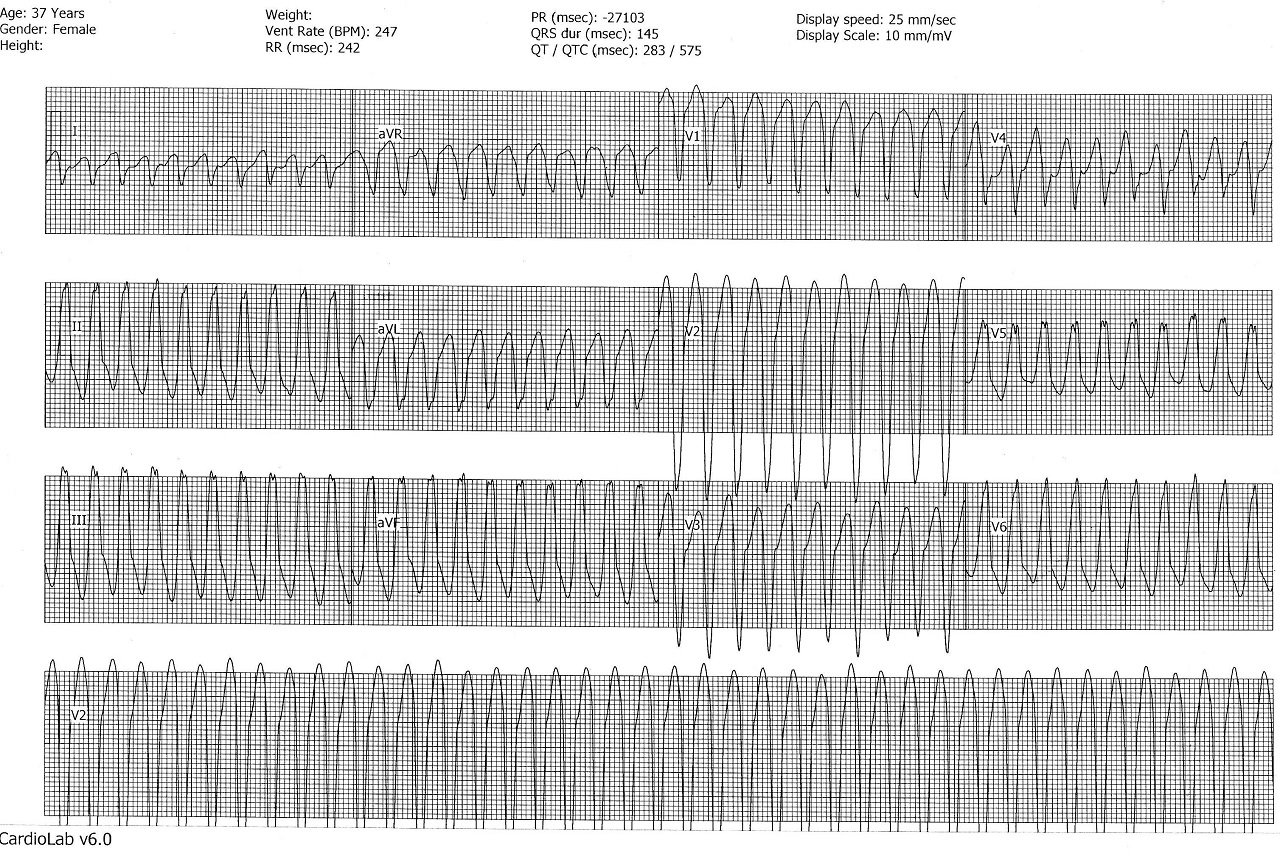
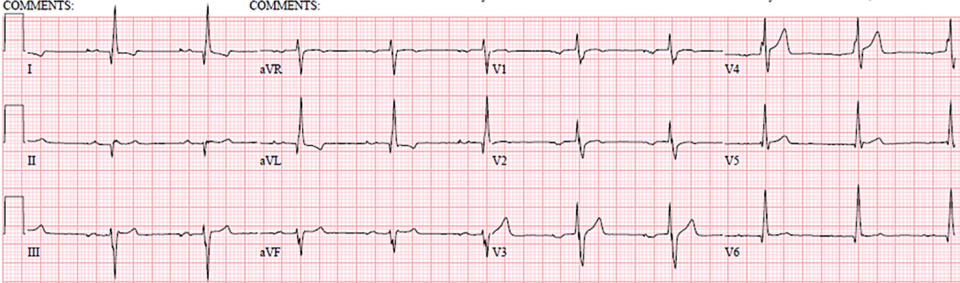
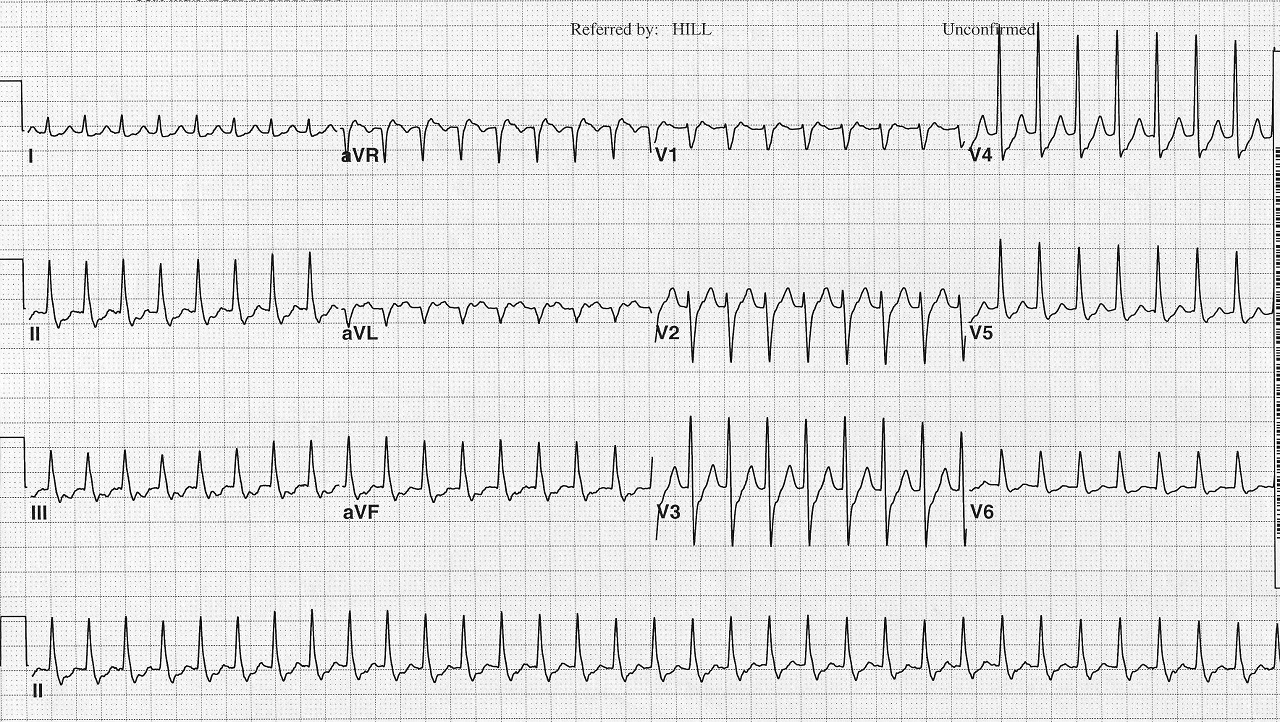 Supraventricular tachycardia (SVT): Narrow complex tachycardia with no clearly visible P wave.
Supraventricular tachycardia (SVT): Narrow complex tachycardia with no clearly visible P wave.
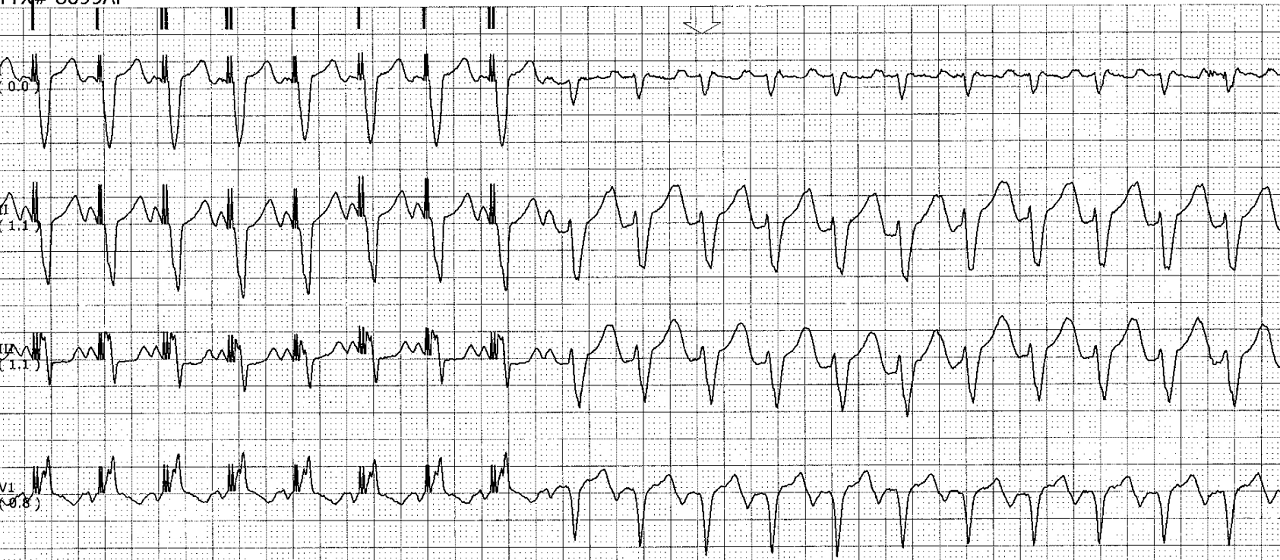
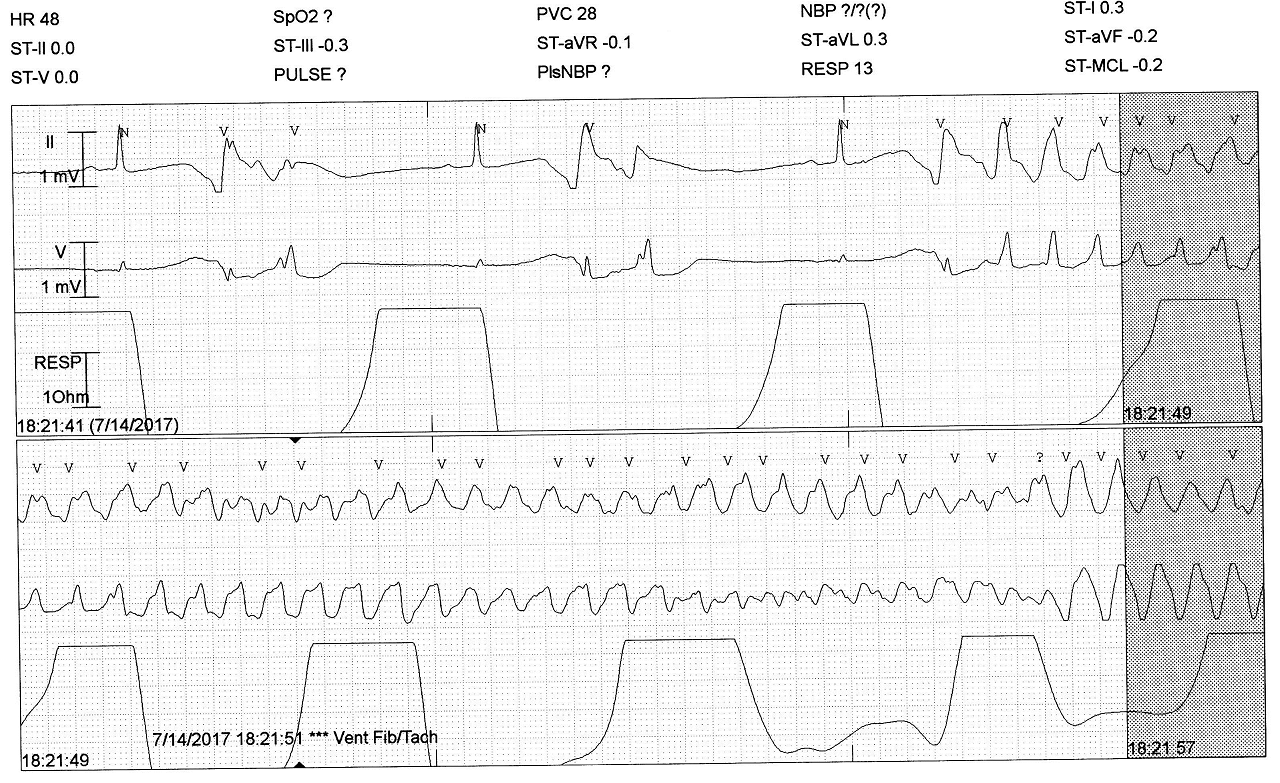 Polymorphic VT with long QT or Torsade de Pointes.
Polymorphic VT with long QT or Torsade de Pointes.
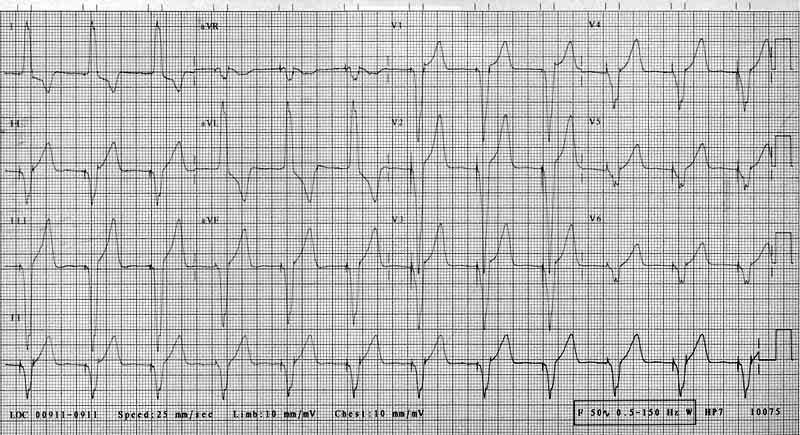
 Idiopathic VT from RV outflow tract. Noted with positive QRS in II, III, and aVF;
normal R wave progression in chest leads.
Idiopathic VT from RV outflow tract. Noted with positive QRS in II, III, and aVF;
normal R wave progression in chest leads.
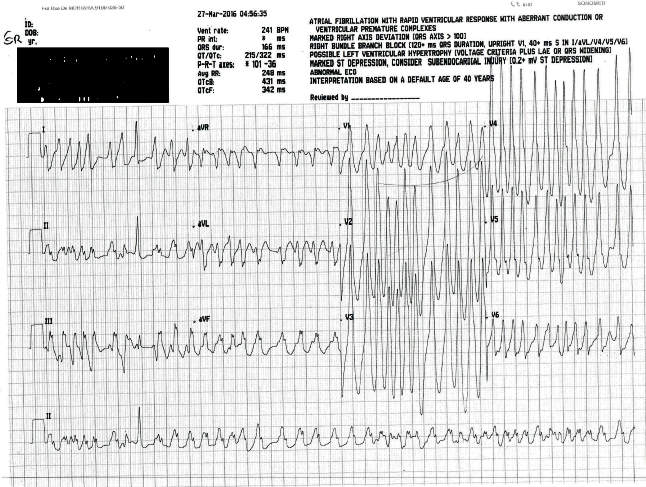
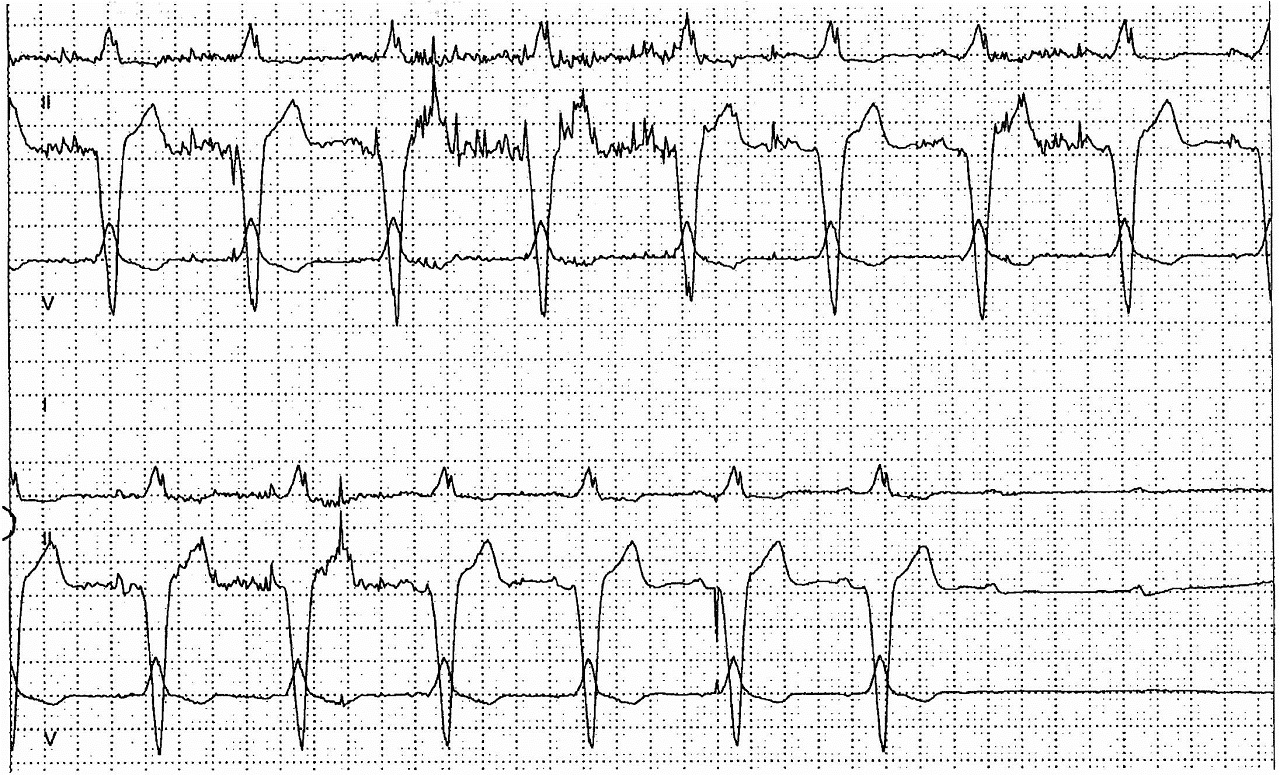
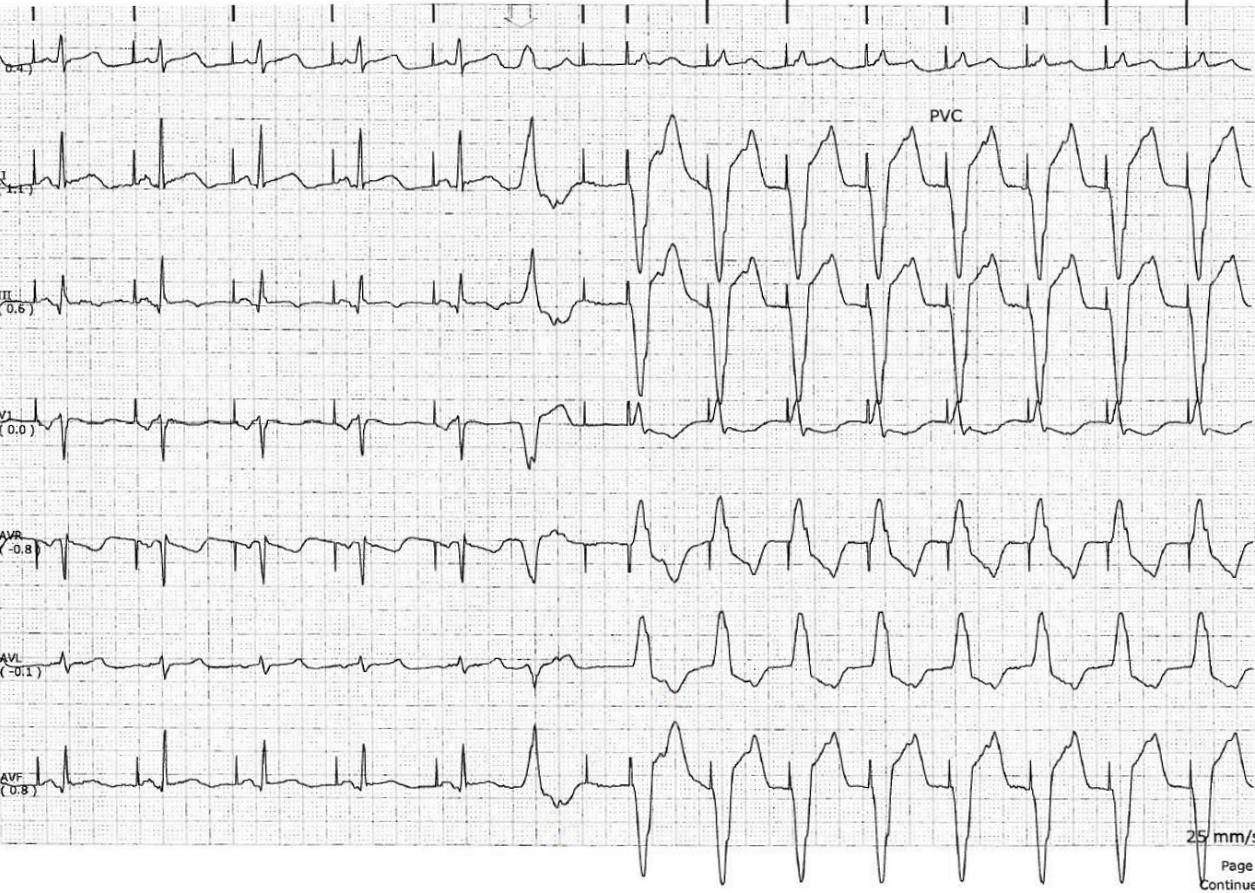
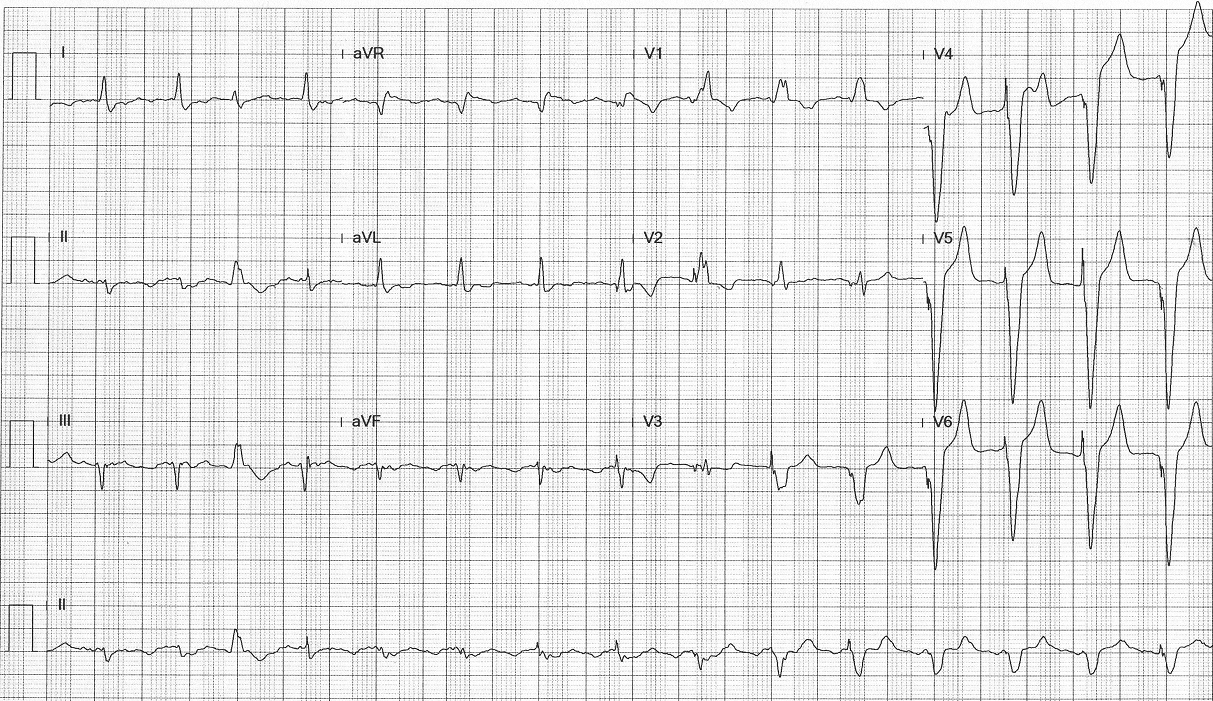
 Ischemic VT in a patient with history of inferior wall MI.
Ischemic VT in a patient with history of inferior wall MI.
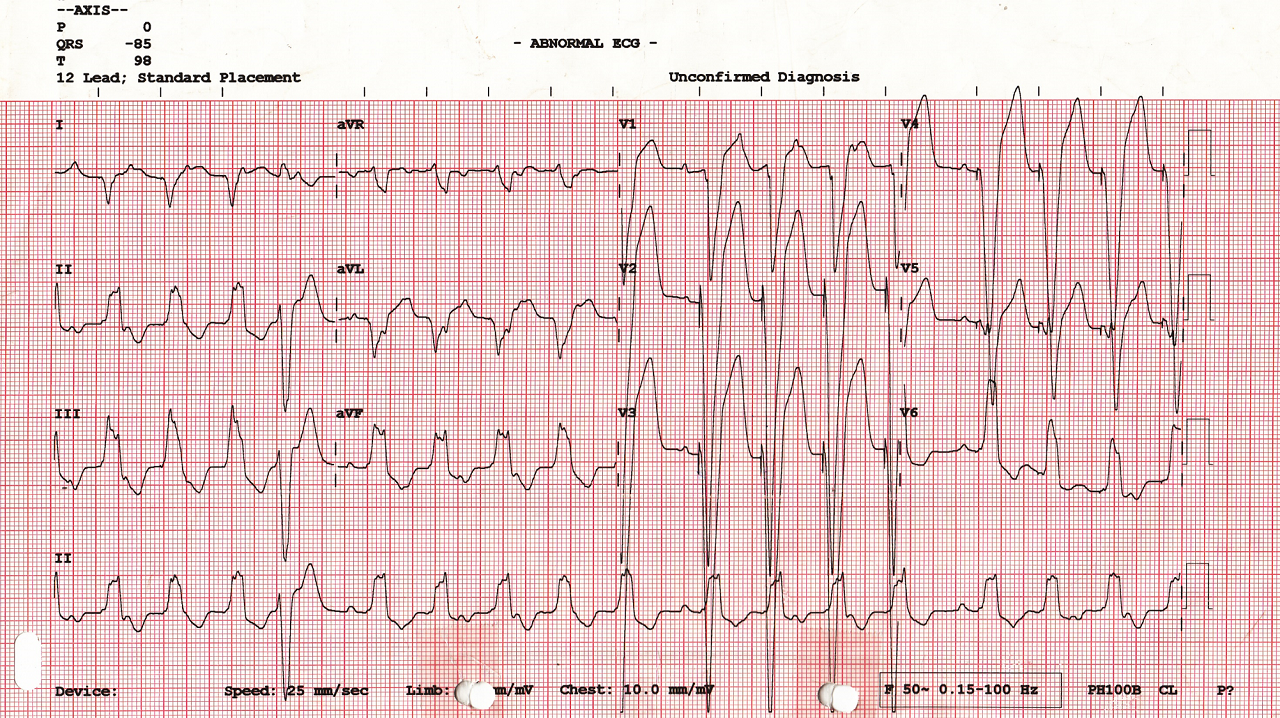
 Monomorphic VT. VA dissociation is clearly seen.
Monomorphic VT. VA dissociation is clearly seen.
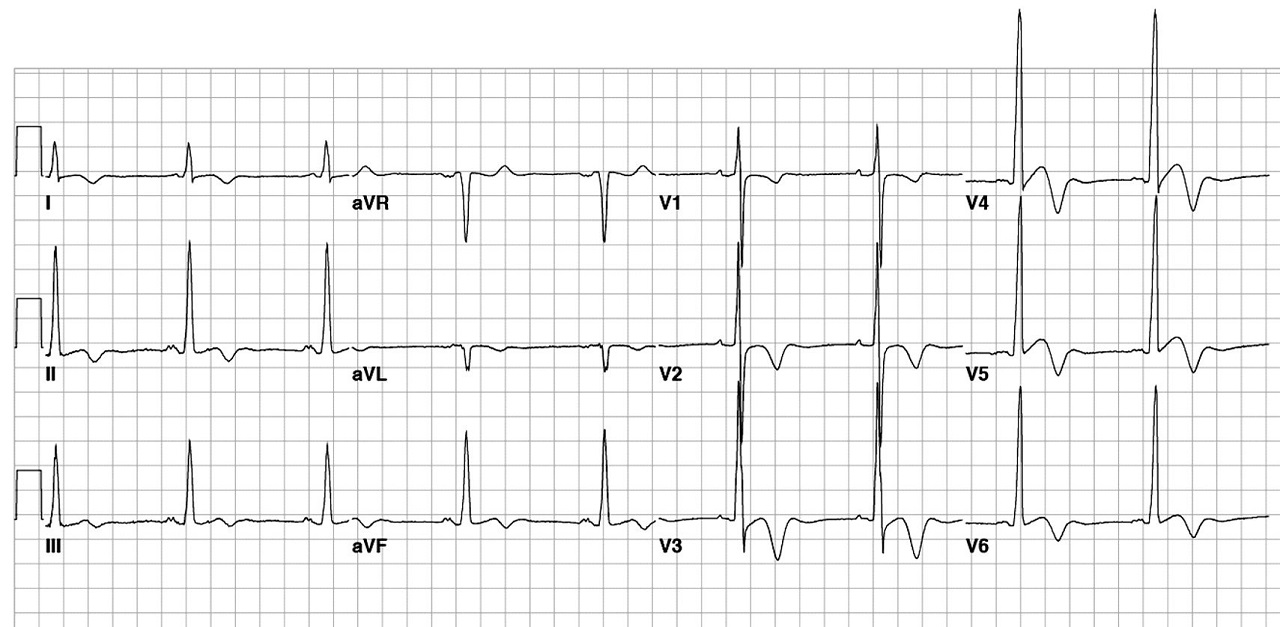
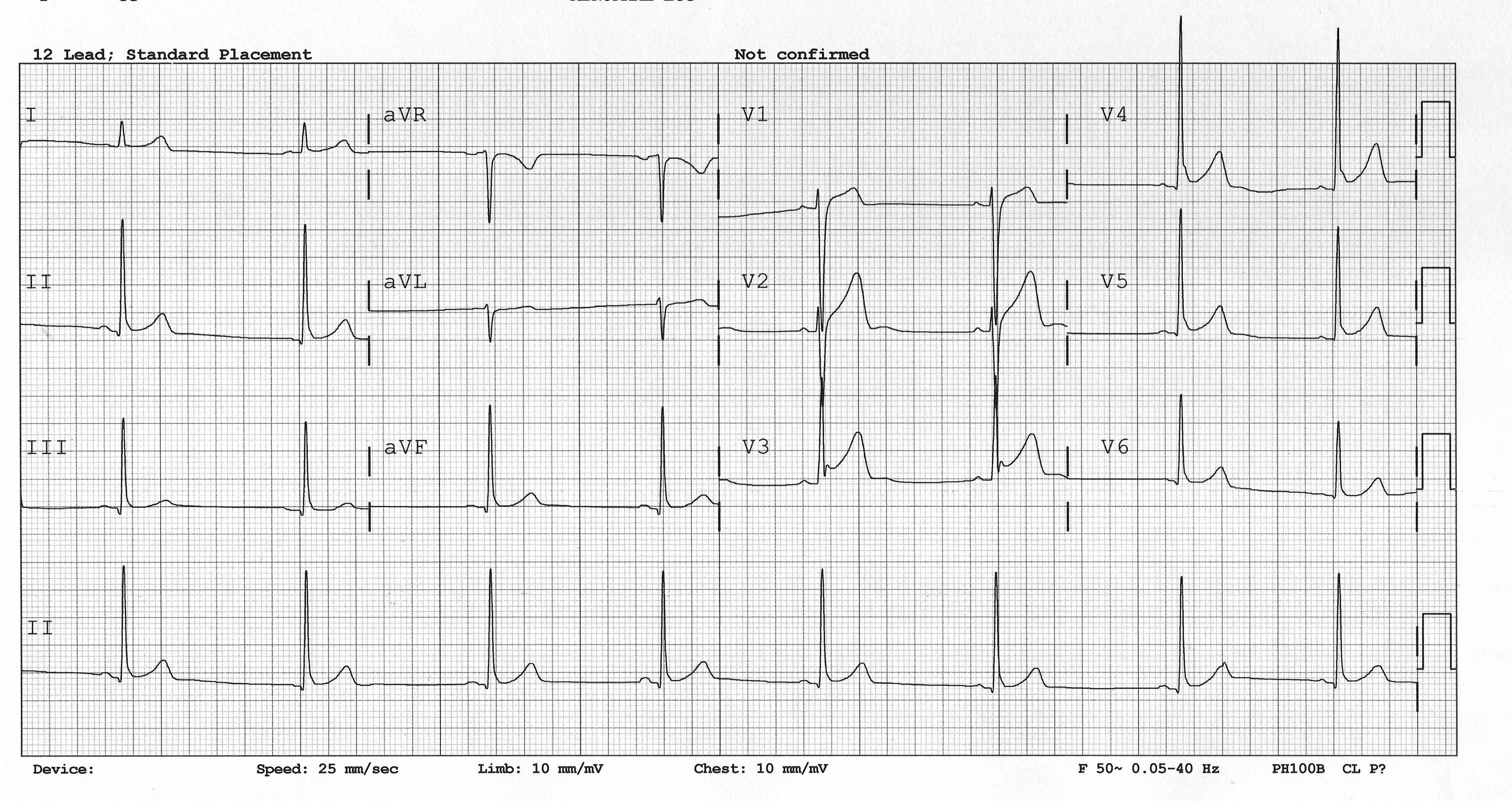
 Brugada ECG: J point elevation with coved-type ST elevation in V1-V2.
Brugada ECG: J point elevation with coved-type ST elevation in V1-V2.
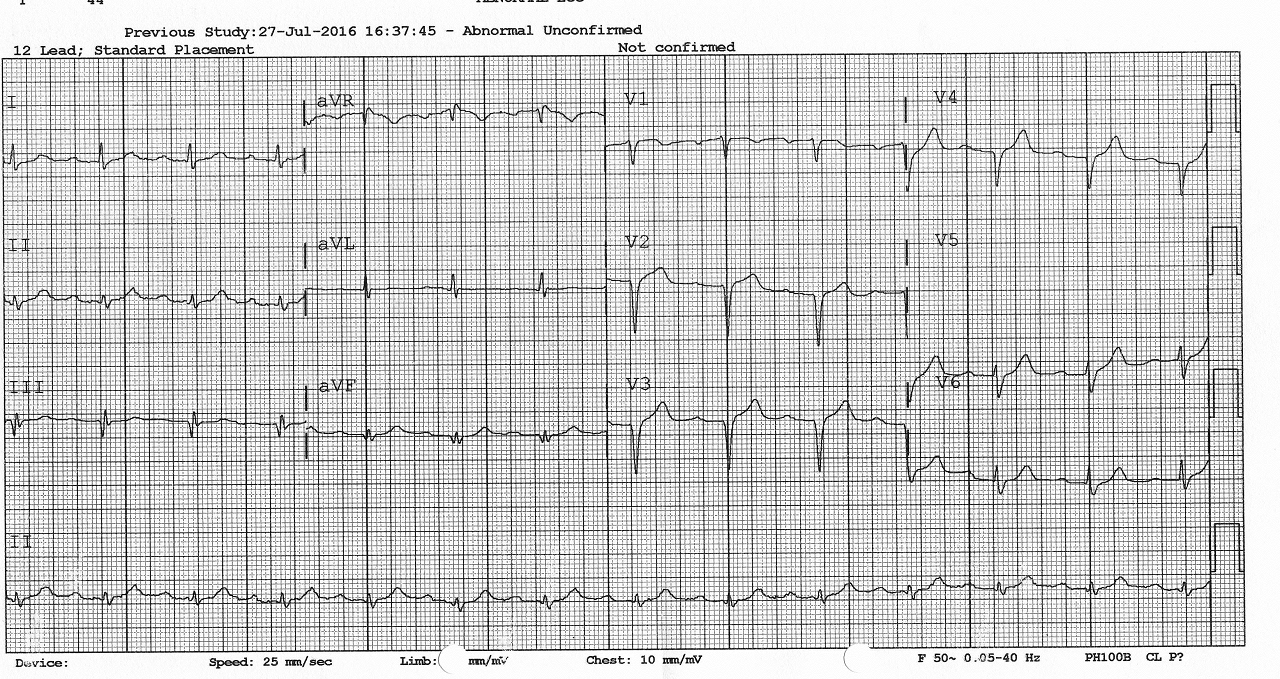
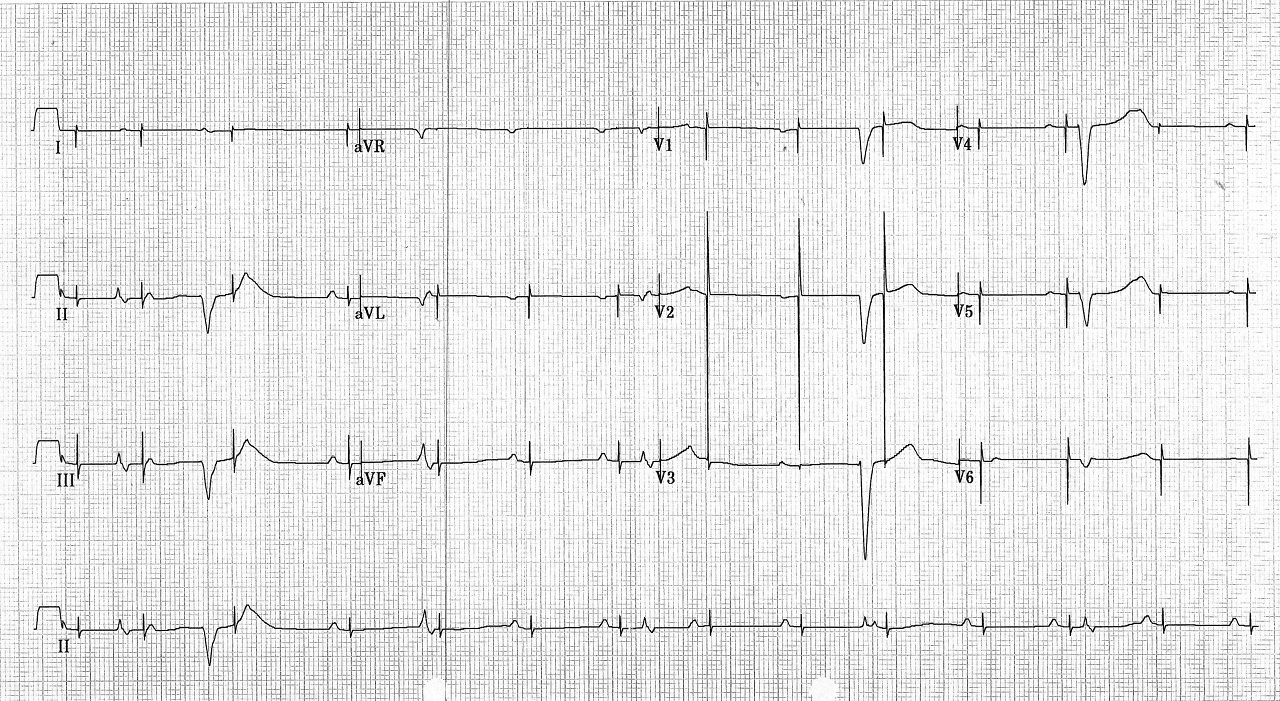
 Hypertrophic cardiomyopathy: high voltage in left-sided leads with ST depression and
T wave inversion.
Hypertrophic cardiomyopathy: high voltage in left-sided leads with ST depression and
T wave inversion.
 Long QT
Long QT
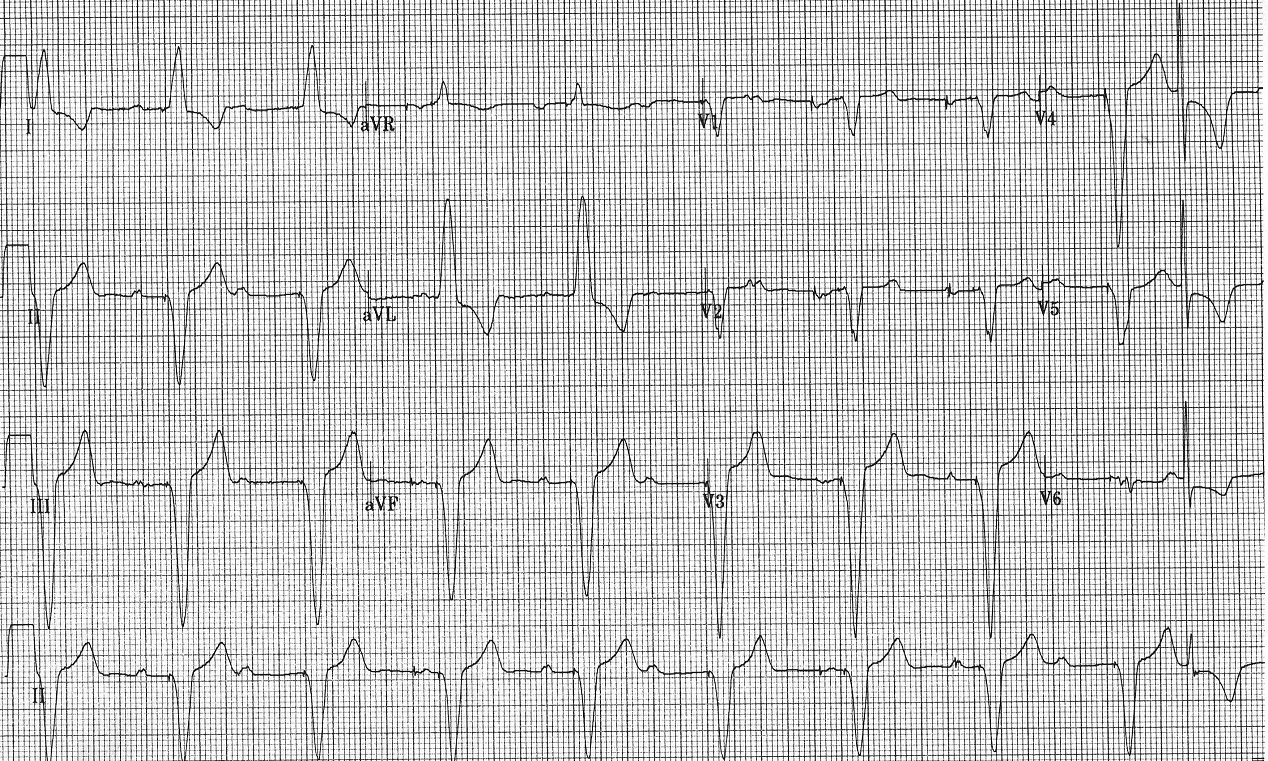
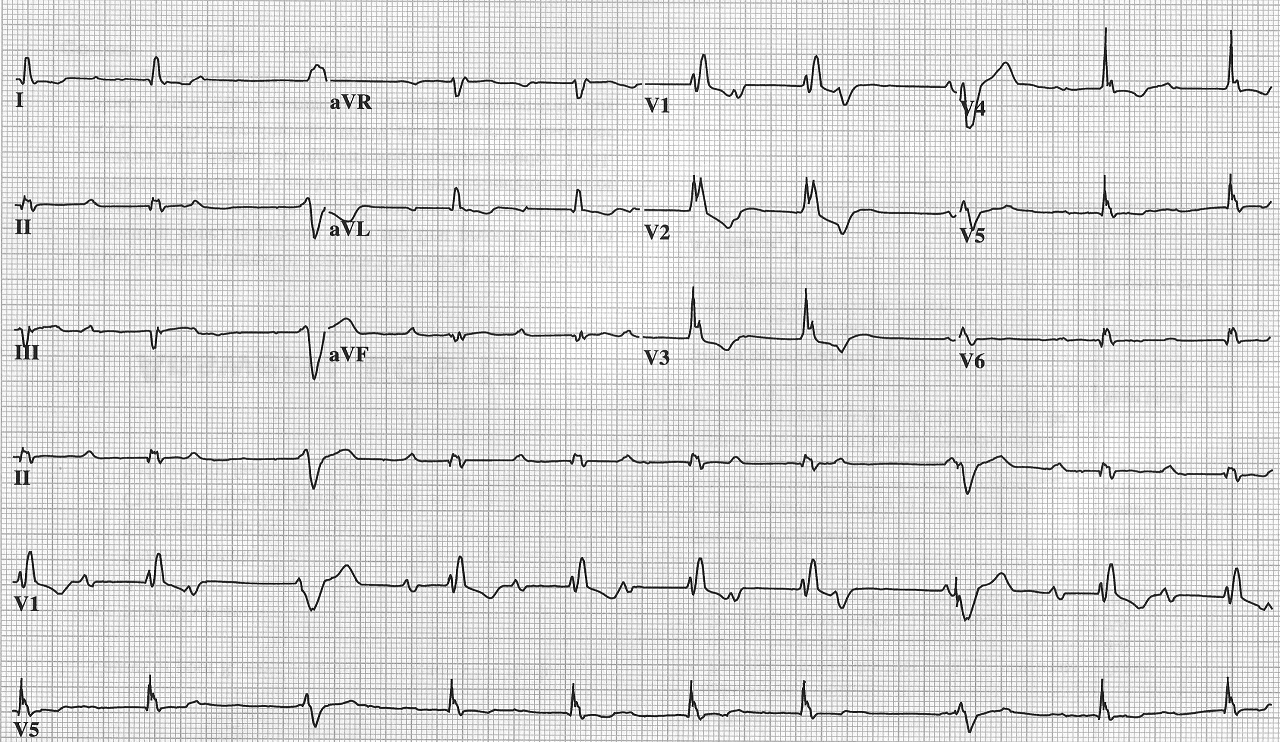
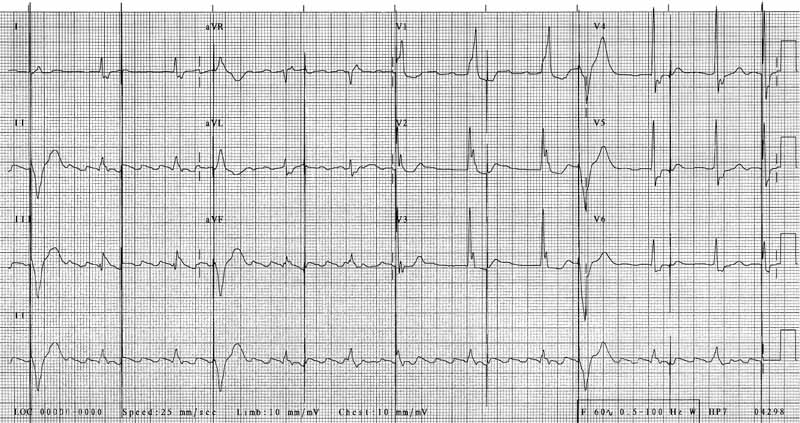
 Old MI; Noted with Q waves in inferior and anterior leads.
Old MI; Noted with Q waves in inferior and anterior leads.
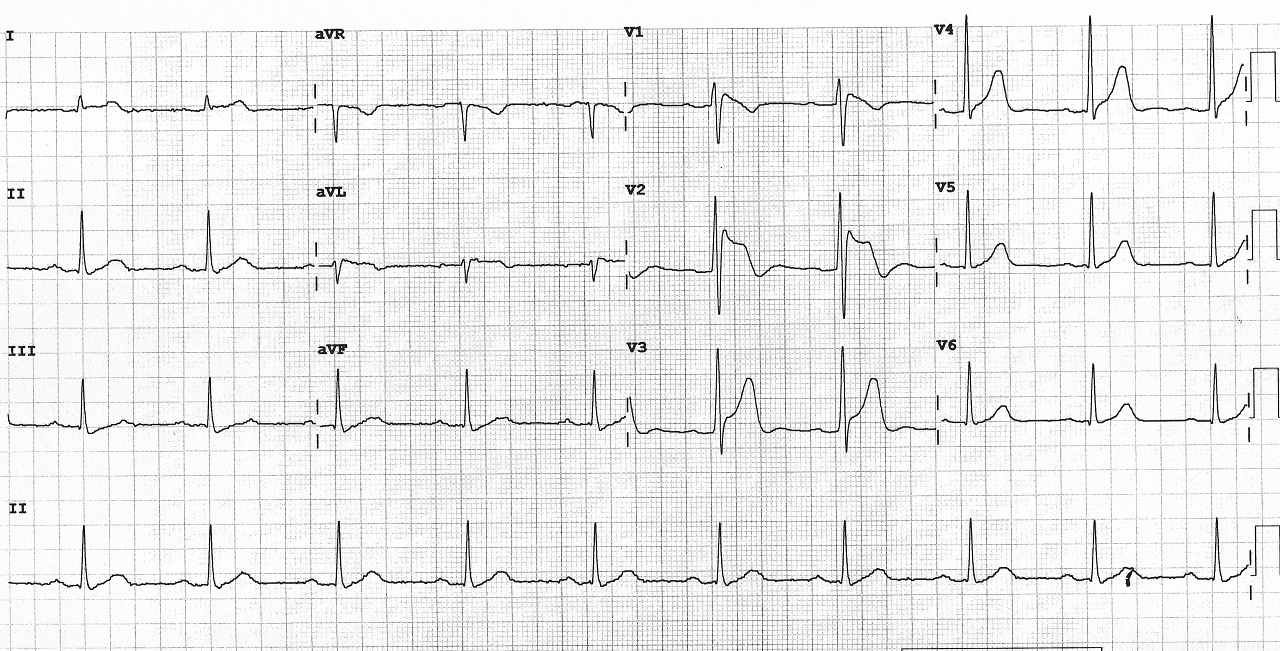
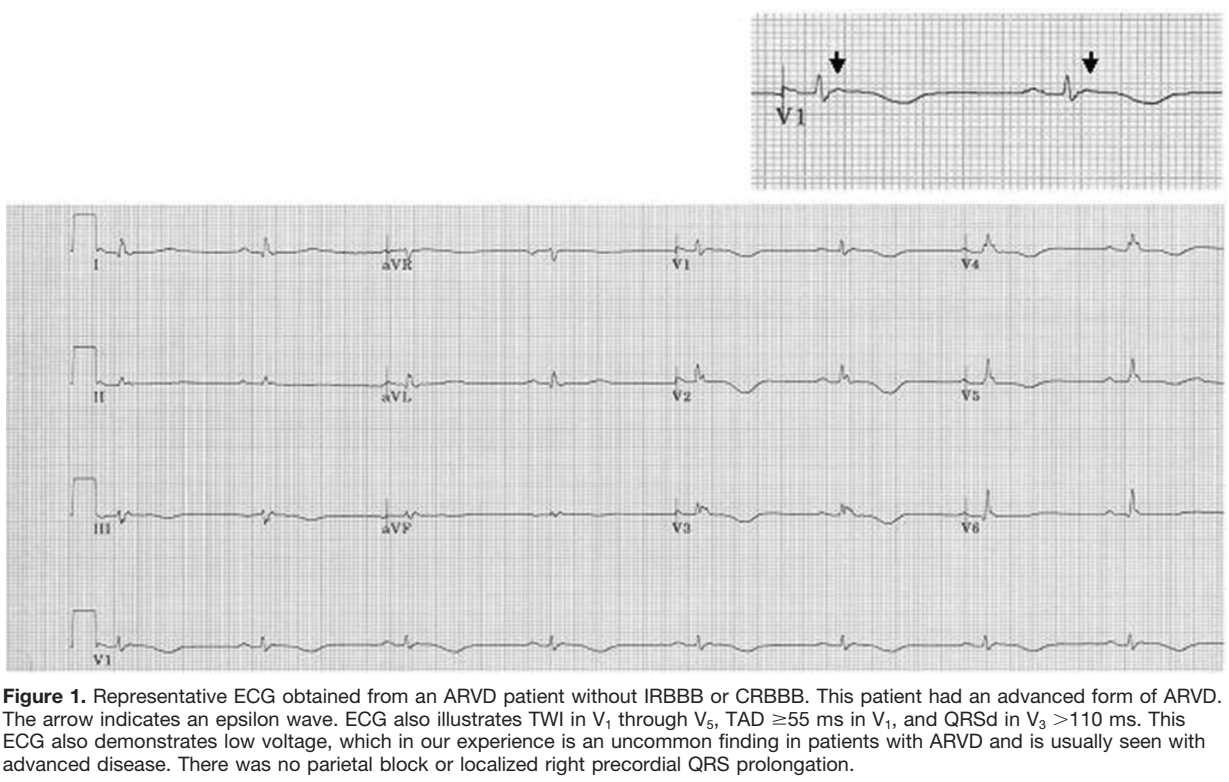 Arrhythmogenic right ventricular dysplasia (ARVD), a disease of right ventricule.
Characteristic ECG findings include Epsilon wave (delay in depolarization) and
T wave inversion in V1-V4.
Arrhythmogenic right ventricular dysplasia (ARVD), a disease of right ventricule.
Characteristic ECG findings include Epsilon wave (delay in depolarization) and
T wave inversion in V1-V4.
 Early repolarization: J point elevation concaved downward ST elevation.
Early repolarization: J point elevation concaved downward ST elevation.
 Short QT
Short QT
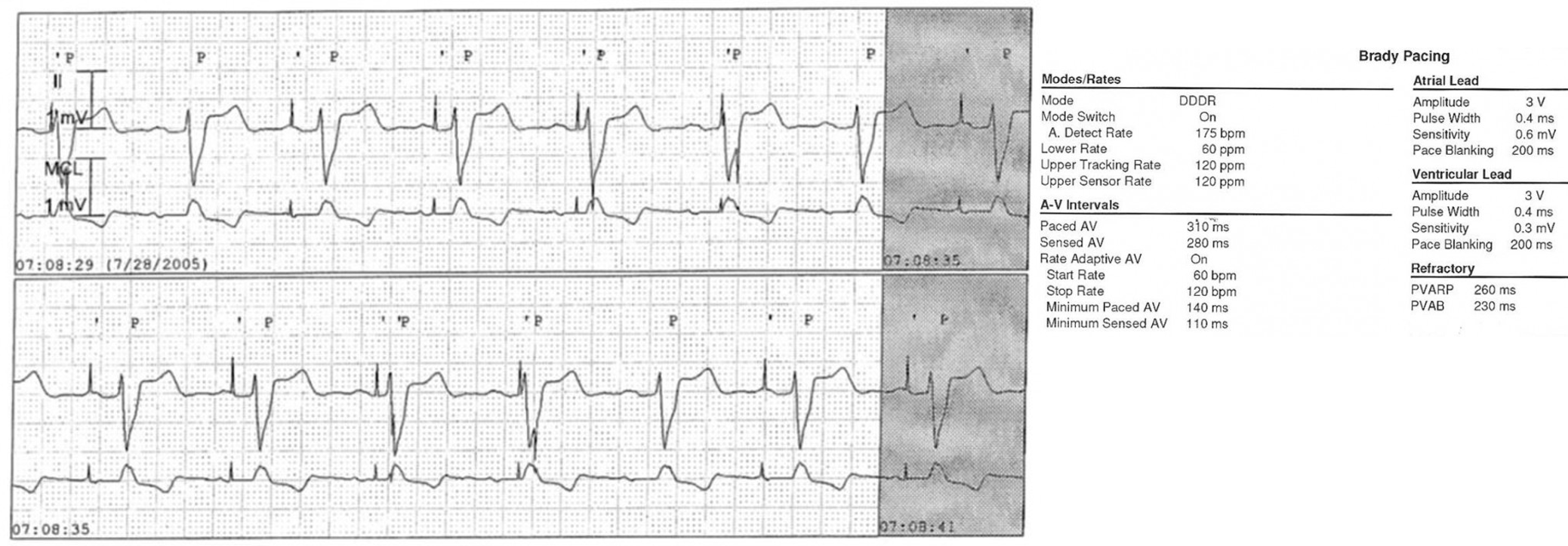
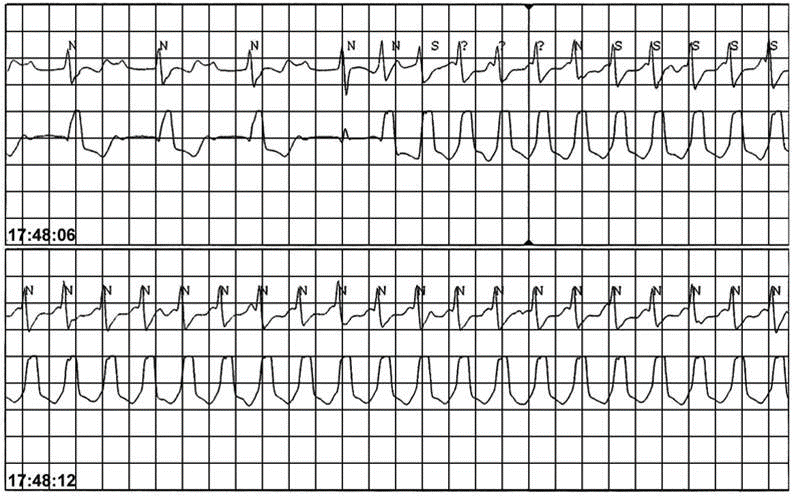
 A and V leads switch in the header. Ventricular pacing is being inhibited by P wave (middle tracing),
ruling out lead dislodgement (there needs to be a lead in atrium).
Inhibition of V pacing is intermittent due to higher sensitivity in A channel.
A and V leads switch in the header. Ventricular pacing is being inhibited by P wave (middle tracing),
ruling out lead dislodgement (there needs to be a lead in atrium).
Inhibition of V pacing is intermittent due to higher sensitivity in A channel.
 Intermittent failure to pace the ventricle is noted. Oversensing is suspected.
Intermittent failure to pace the ventricle is noted. Oversensing is suspected.
 Normal pacemaker function. DDI 60, AVD 200.
Normal pacemaker function. DDI 60, AVD 200.
 Normal pacemaker function. Rhythm = sinus rhythm with AV Wenckebach.
V pacing came on the dropped beats.
Normal pacemaker function. Rhythm = sinus rhythm with AV Wenckebach.
V pacing came on the dropped beats.
 Pacemaker mediated tachycardia; triggered by a PVC with retrograde P, followed
by an non-capture A pacing with long AV delay, allowing the following retrograde
VA conduction to capture the atrium and initiate PMT.
Pacemaker mediated tachycardia; triggered by a PVC with retrograde P, followed
by an non-capture A pacing with long AV delay, allowing the following retrograde
VA conduction to capture the atrium and initiate PMT.
 Sinus tachycardia with pacemaker Wenckebach.
Sinus tachycardia with pacemaker Wenckebach.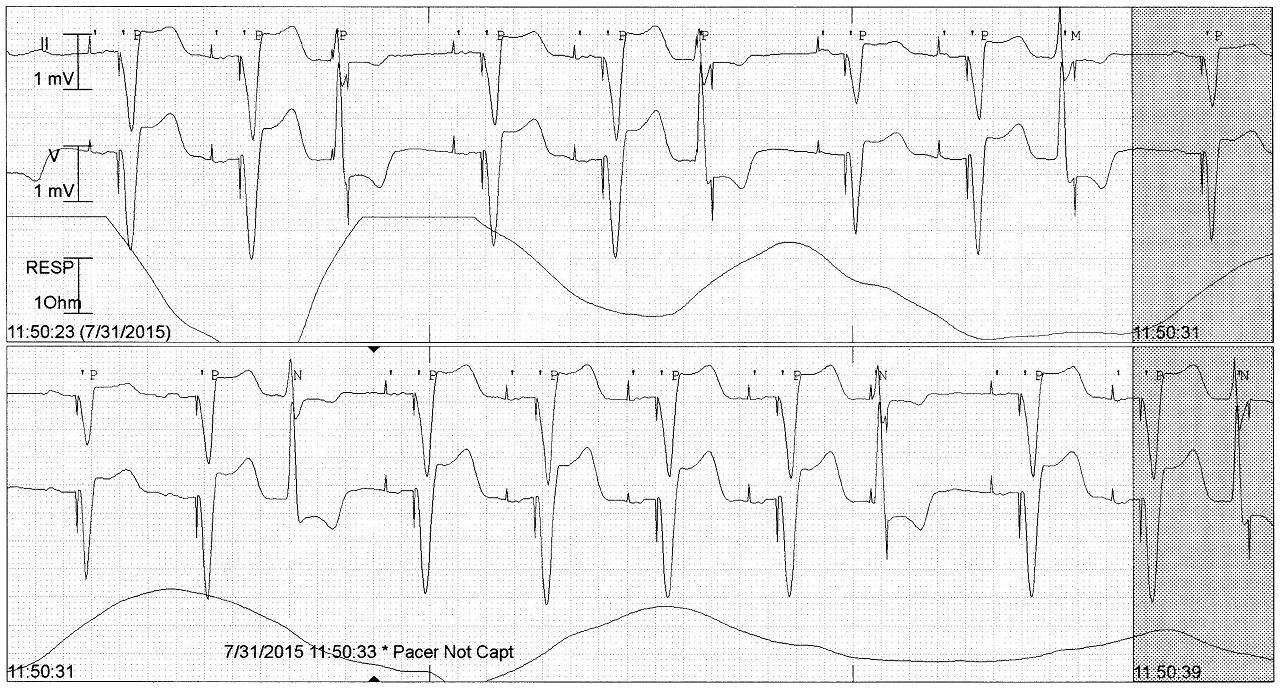 Safety pacing triggered by timely PVCs. Noted with short AV delays.
Safety pacing triggered by timely PVCs. Noted with short AV delays.
 Managed ventricular pacing: AAI mode switches to DDD with short AV delay after
AP without native ventricular beat.
Managed ventricular pacing: AAI mode switches to DDD with short AV delay after
AP without native ventricular beat.
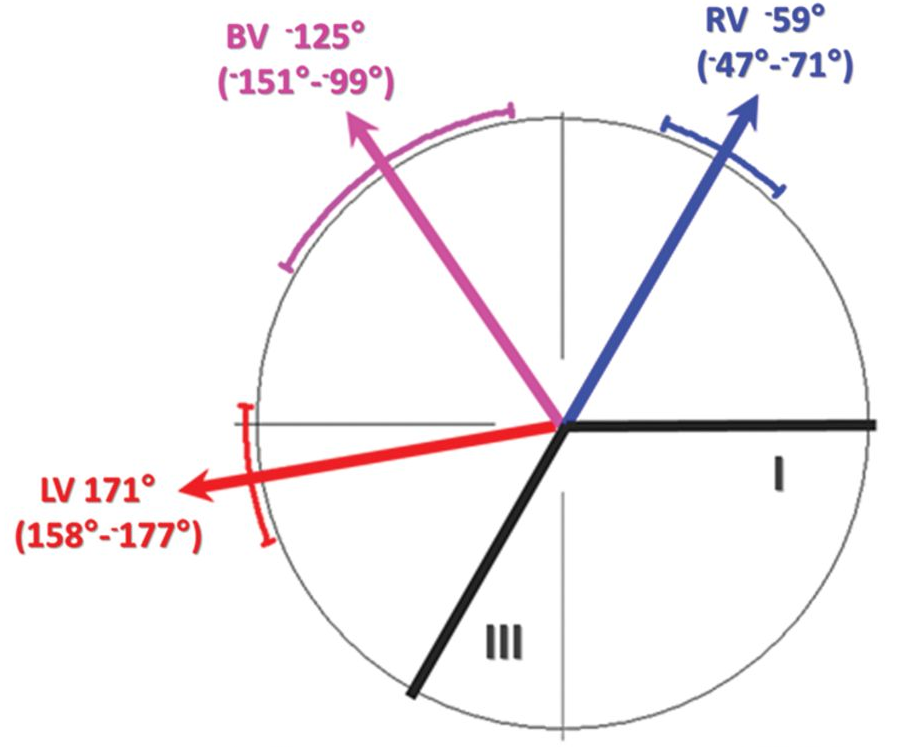
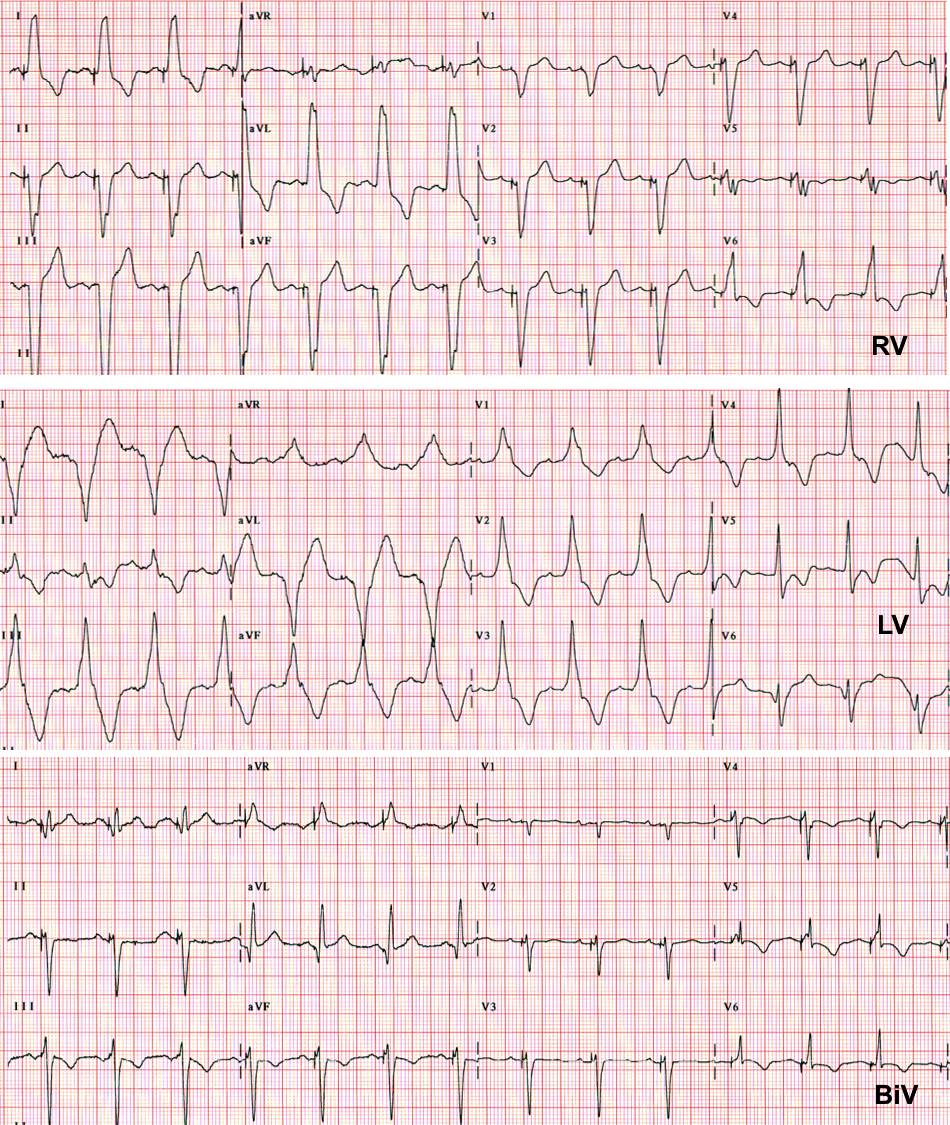
 Sinus tachycardia above upper rate limit; hence no biventricular pacing.
Sinus tachycardia above upper rate limit; hence no biventricular pacing.
 The atrial lead has dislodged into the ventricle. Ventricular captures are seen
by the first spike (from atrial lead) followed by a functional non-capture from the second spike (from
ventricular lead).
The atrial lead has dislodged into the ventricle. Ventricular captures are seen
by the first spike (from atrial lead) followed by a functional non-capture from the second spike (from
ventricular lead).
 Normal CRT function with VV delay of 40ms.
Normal CRT function with VV delay of 40ms.
 Pacemaker failure. Radiation may cause deterioration of lead and pacemaker
circuit. ECG show asynchronous pacing. Urgent generator change is needed.
Pacemaker failure. Radiation may cause deterioration of lead and pacemaker
circuit. ECG show asynchronous pacing. Urgent generator change is needed.